 2015, Vol. 17
2015, Vol. 17



肺炎链球菌(Streptococcus pneumoniae, SP)是导致婴幼儿严重疾病的首要因素,也是引起肺炎、鼻窦炎和急性中耳炎的最常见病原[1]。机体抵抗力低下时,SP侵入正常无菌部位引起败血症、脑膜炎、腹膜炎、关节炎等侵袭性感染,称为侵袭性肺炎链球菌疾病(invasive pneumococcal disease, IPD)。IPD作为疫苗可预防性疾病,在儿童中发病率较高,造成的经济负担较为严重。1999年到2010年亚太地区每年每100 000例小于2岁儿童中约有100~200例确诊为IPD[2]。基于医院的回顾性分析显示南亚住院患儿IPD的发病率为3.57%[3]。奥地利报道小于5岁的IPD患儿17%在出院时并没有完全康复,大部分遗留有耳聋或运动功能缺陷;超过6个月仍有13%的病人存在后遗症[4]。我国因SP感染导致的5岁以下死亡儿童约占该年龄段所有死亡人数的16.5%[5]。IPD已成为世界范围内严重的公共卫生问题,许多国家建立了SP或IPD监测系统,但我国的监测系统不完善,对侵袭性与非侵袭性SP菌株的耐药性差异研究较少。本研究对温州医科大学附属育英儿童医院SP感染病例进行5年的监测,通过对照分析侵袭性与非侵袭性SP菌株的药敏资料,了解两类菌株的耐药性差异,为合理使用抗菌药物治疗不同类型SP感染提供依据。
1 资料与方法 1.1 研究对象选取2009年1月1日至2013年12月31日于温州医科大学附属育英儿童医院就诊的70例IPD患儿为研究对象,其中男40例,女30例,年龄范围0~14岁,<2岁32例,2~5岁25例,>5岁13例。IPD诊断标准参照文献[6]。同时按1 : 2对照研究方法,随机选取同期(1年内)因SP所致下呼吸道感染住院的164例患儿为对照组,其中男92例,女72例,年龄范围0~14岁,<2岁80例,2~5岁71例,>5岁13例。
1.2 细菌检测及药敏试验(1)分离培养:采集IPD患儿血液、脑脊液、胸腹腔积液、纵隔及软组织引流液、中段尿标本送检;采集对照组患儿痰液标本送检。将标本接种于5%绵羊血琼脂平板,置35℃、7%CO2培养箱中培养18~24 h。
(2)菌种鉴定:挑选血平板上的可疑菌落进一步分离纯化,同时做奥普托欣(Optochin)试验,然后再用VITEK32全自动微生物分析仪(法国梅里埃公司)和GPI卡鉴定到种。
(3)药敏试验:应用MSTRP+I板条在MicroScan Walk Away 96 SI检测;判断标准参照美国临床和实验室标准委员会(CLSI)2008年版标准[7]。SP质控菌株ATCC 49619购自卫生部临检中心。多重耐药为同时对三类或者三类以上的抗菌药物耐药。
1.3 统计学分析采用SPSS 19.0统计软件对数据进行统计学分析,计数资料采用百分率(%)表示,组间比较采用卡方检验,P<0.05为差异有统计学意义。
2 结果 2.1 侵袭性SP的分离情况从70例IPD患儿的无菌部位共分离到82株侵袭性SP,其中分离自血液49株(60%),脑脊液19株(23%),臀部等软组织8株(10%),胸腹水4株(5%),中段尿2株(2%)。其中6例同时检出血液、脑脊液培养阳性,2例同时检出血液、胸水培养阳性,1例1次血培养和2次脑脊液培养阳性,1例2次脑脊液培养阳性,1例2次血培养阳性。
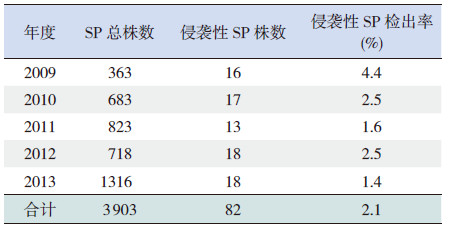
2.2 侵袭性SP检出率的年度变化2009~2013年间SP检出菌株数呈明显增加趋势,而侵袭性SP的检出率呈下降趋势(χ2=14.994, P<0.01),其中2011年、2013年的侵袭性SP检出率较2009年明显下降(分别χ2=13.252、8.446,P<0.01)。见表 1。
| 表 1 2009~2013 年侵袭性SP 检出情况比较 |
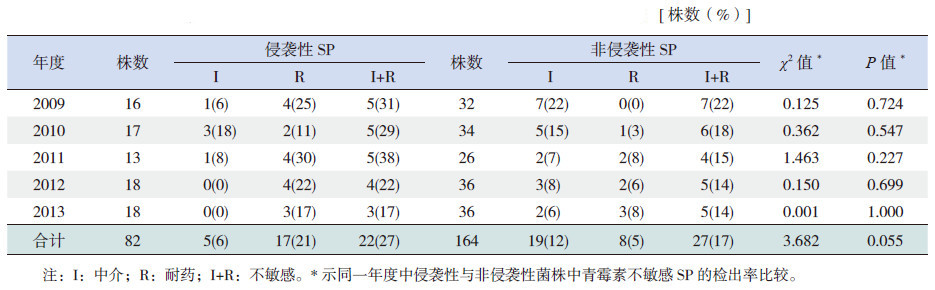
从对照组患儿标本中共分离到非侵袭性SP 164株,按照2008年CLSI的药敏新折点[7],侵袭性与非侵袭性菌株中青霉素不敏感SP(PNSP)的检出比例均较低,分别为27%和17%(χ2=3.682,P>0.05),但脑脊液标本中侵袭性PNSP检出率(89%,17/19)明显高于其他标本中侵袭性PNSP检出率(8%,5/63)(χ2=54.284,P<0.01);侵袭性菌株中青霉素耐药SP(PRSP)共17株,全部分离自脑脊液;而5株青霉素中介SP(PISP)全部分离自血液。同一年度中侵袭性与非侵袭性菌株中PNSP检出率的差异均无统计学意义(P>0.05)。各年度侵袭性SP中,PNSP检出率差异无统计学意义(χ2=2.255,P>0.05)。见表 2。
| 表 2 各年度侵袭性与非侵袭性SP 对青霉素的不敏感率比较 |
82株侵袭性SP中,PNSP对头孢噻肟、头孢曲松、头孢吡肟的不敏感率均明显高于青霉素敏感SP(PSSP),差异有统计学意义(P<0.01)。见表 3。
| 表 3 侵袭性SP 中PNSP 与PSSP 对其他抗菌药物的不敏感率比较 |

侵袭性与非侵袭性SP对大环内酯类抗生素的耐药率均超过97%;对复方新诺明、头孢克洛、头孢呋辛的不敏感率超过79%,对氯霉素、头孢吡肟、阿莫西林/克拉维酸的不敏感率低于40%,未发现对万古霉素和左氧氟沙星耐药的SP。其中侵袭性SP对头孢噻肟、头孢曲松的不敏感率显著高于非侵袭性SP,对美罗培南的不敏感率显著低于非侵袭性SP(P<0.05)(表 4)。进一步分析发现,脑脊液与非脑脊液侵袭性SP对头孢噻肟的不敏感率(63% vs 21%)和头孢曲松的不敏感(76% vs 12%)比较差异均有统计学意义(分别χ2=12.455、22.359,P<0.05)。侵袭性与非侵袭性SP的多重耐药率分别为89%和93%(χ2=1.333,P>0.05),主要对大环内酯类、二代头孢类、四环素类及复方新诺明耐药。
3 讨论美国学者报道小于5岁儿童侵袭性SP的检出率由1999~2000年的29%下降为2010~2011年的20%~21%,其中血液中SP检出率由31%下降为23%~25%[8];另有学者报道2004~2005年<2岁儿童SP脑膜炎的发病率比1998~1999年下降了64%[9];加拿大<5岁IPD患儿发病率也有所下降[10]。IPD发病率下降考虑与SP疫苗使用有关。本研究显示,我院2009~2013年侵袭性SP的检出率呈下降趋势,本组患儿无1例接种SP疫苗,出现下降的原因可能与SP总检出数增多有关,其中2013年SP检出数为2009年的3.6倍。
自1967年澳大利亚首次报道PRSP以来,SP耐药形势日趋严峻。采用旧的CLSI青霉素耐药折点,美国报道PNSP检出率由1999~2000年的33%增加到2010~2011年的39%[8]。本院2009~2012年分离自血液的菌株中PNSP高达96%[11]。然而采用2008年新的CLSI青霉素耐药折点后,非脑脊液标本中SP对青霉素的耐药率明显下降[12, 13, 14]。姚开虎等[15]报道2006~2007年北京、上海、广州、深圳4个地区儿童SP中PNSP为86%,中国CHINET 细菌耐药监测显示2007年北京、上海、广州等地区儿童痰液中 PNSP为88.5%(PISP 69.2%,PRSP19.3%),2012年则降至22.9%(PISP12.7%,PRSP10.2%)[16, 17]。我院儿童侵袭性SP中PNSP由2004~2009年的71%[18]下降为2009~2013年的27%(PRSP 21%,PISP 6%);同时痰液中PNSP的检出率由2004~2007年的83%[19]下降为本研究的17%(PRSP 5%,PISP 12%)。考虑主要与青霉素折点改变有关,另外还可能与较少使用青霉素治疗SP感染,以致仍保持较高敏感性有关。脑脊液中PRSP检出率明显高于非脑脊液中检出率,可能与不同部位青霉素折点判断标准不同有关。
本研究进一步发现,侵袭性菌株中PNSP对头孢噻肟、头孢曲松、头孢吡肟的不敏感率均高于PSSP菌株,与Choi等[20]的报道一致。其原因可能与头孢菌素的不敏感率多发生于青霉素不敏感之后,青霉素结合位点的多次突变导致SP对第三、四代头孢菌素的不敏感有关[20]。
本组侵袭性与非侵袭性SP对头孢克洛、头孢呋辛的不敏感率均超过80%,考虑与广泛使用二代头孢菌素有关。侵袭性SP对头孢噻肟、头孢曲松的不敏感率明显高于非侵袭性SP,主要原因是脑脊液中对头孢噻肟、头孢曲松不敏感的SP所占比例较高(分别为48%与63%)。本组资料中侵袭性和非侵袭性SP对红霉素、阿奇霉素的不敏感率均超过97%,因此,当临床怀疑或者明确为SP感染时,不应选择大环内酯类抗生素治疗。侵袭性与非侵袭性SP对阿莫西林/克拉维酸的不敏感率均较低,可以选择阿莫西林/克拉维酸治疗除脑膜炎外的SP感染。侵袭性SP的多重耐药率为89%,与本院2009年前的报道相近[18],稍低于Liu等[21]报道的95.6%。痰液中SP的多重耐药率为93%,主要对大环内酯类、二代头孢菌素、四环素类及复方新诺明耐药。显示SP的多重耐药形势严峻,应合理使用抗菌药物,加强医院感染防控,以延缓耐药。
总之,本院2009~2013年侵袭性SP菌株的检出率呈下降趋势。虽然侵袭性与非侵袭性SP对青霉素的不敏感率低于30%,但脑脊液中PNSP检出率接近90%,因此青霉素不应用于SP脑膜炎的治疗。对大环内酯类、二代头孢菌素的不敏感率高于80%,不建议使用大环内酯类及二代头孢菌素治疗SP感染。侵袭性菌株中PNSP对头孢噻肟、头孢曲松、头孢吡肟的不敏感率明显高于PSSP,且均超过60%,因此,当侵袭性SP菌株对青霉素不敏感时,不应选择上述三、四代头孢菌素治疗IPD。
| [1] | 罗圆, 怀扬, 余宏杰. 发展中国家侵袭性肺炎链球菌病监测研究进展[J]. 中华流行病学杂志, 2010, 31(7): 816-819. |
| [2] | Lin TY, Shah NK, Brooks D, et al. Summary of invasive pneumococcal disease burden among children in the Asia- Pacific region[J]. Vaccine, 2010, 28(48): 7589-7605. |
| [3] | Jaiswal N, Singh M, Thumburu KK, et al. Burden of invasive pneumococcal disease in children aged 1 month to 12 years living in South Asia: a systematic review[J]. PLoS One, 2014, 9(5): e96282. |
| [4] | Paulke-Korinek M, Kollaritsch H, Kundi M. Characteristics of invasive pneumococcal disease in hospitalized children in Austria[J]. Eur J Pediatr, 2014, 173(4): 469-476. |
| [5] | Rudan L, Chan KY, Zhang JS, et al. Causes of deaths in children younger than 5 years in China in 2008[J]. Lancet, 2010, 375(9720): 1083-1089. |
| [6] | Gaschignard J, Levy C, Chrabieh M, et al. Invasive pneumococcal disease in children can reveal a primary immunodeficiency[J]. Clin Infect Dis, 2014, 59(2): 244-251. |
| [7] | Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing, Eighteenth informational supplement. CLSI document M100-S18[S]. Wayne, Pennsylvania: 2008: 1-181. |
| [8] | Richter SS, Heilmann KP, Dohrn CL, et al. Pneumococcal serotypes before and after introduction of conjugate vaccines, United States, 1999-2011[J]. Emerg Infect Dis, 2013, 19(7): 1074-1083. |
| [9] | Hsu HE, Shutt KA, Moore MR, et al. Effect of pneumococcal conjugate vaccine on pneumococcal meningitis[J]. N Engl J Med, 2009, 360(3): 244-256. |
| [10] | Kuster SP, Rudnick W, Shigayeva A, et al. Previous antibiotic exposure and antimicrobial resistance in invasive pneumococcal disease: results from prospective surveillance[J]. Clin Infect Dis, 2014, 59(7): 944-952. |
| [11] | 苏小燕, 温顺航, 林立, 等. 儿童肺炎链球菌败血症的临床特点及药敏分析[J]. 中国当代儿科杂志, 2013, 15(11): 995-999. |
| [12] | Su LH, Wu TL, Kuo AJ, et al. Antimicrobial susceptibility of Streptococcus pneumoniae at a university hospital in Taiwan, 2000-07: impact of modified non-meningeal penicillin breakpoints in CLSI M100-S18[J]. J Antimicrob Chemother, 2009, 64(2): 336-342. |
| [13] | Imohl M, Reinert RR, der Linden M. New penicillin susceptibility breakpoints for Streptococcus pneumoniae and their effects on susceptibility categorisation in Germany (1992- 2008) [J]. Int J Antimicrob Agents, 2009, 34(3): 271-273. |
| [14] | Dogan O, Gulmez D, Hascelik G. Effect of new breakpoints proposed by Clinical and Laboratory Standards Institute in 2008 for evaluating penicillin resistance of Streptococcus pneumoniae in a Turkish University Hospital[J]. Microb Drug Resist, 2010, 16(1): 39-41. |
| [15] | 姚开虎, 王立波, 赵根明, 等. 四家儿童医院住院肺炎病例肺炎链球菌分离株的耐药性监测[J]. 中国当代儿科杂志, 2008, 10(3): 275-279. |
| [16] | 王传清, 薛建昌, 张泓, 等. 2007 年全国CHINET 链球菌属分布及耐药性监测[J]. 中国感染与化疗杂志, 2009, 9(3): 180- 184. |
| [17] | 汪复, 朱德妹, 胡付品, 等. 2012 年中国CHINET 细菌耐药性监测[J]. 中国感染与化疗杂志, 2013, 13(6): 321-330. |
| [18] | 刘素云, 董琳, 杨锦红. 儿童侵袭性肺炎链球菌病的临床特征及耐药性分析[J]. 中华儿科杂志, 2010, 48(2): 95-99. |
| [19] | 张丽亚, 董琳. 2004-2007 年温州地区下呼吸道感染患儿肺炎链球菌耐药性分析[J]. 实用儿科临床杂志, 2009, 24(10): 765-767. |
| [20] | Choi SH, Chung JW, Sung H, et al. Impact of penicillin nonsusceptibility on clinical outcomes of patients with nonmeningeal Streptococcus pneumoniae bacteremia in the era of the 2008 clinical and laboratory standards institute penicillin breakpoints[J]. Antimicrob Agents Chemother, 2012, 56(9): 4650-4655. |
| [21] | Liu C, Xiong X, Xu W, et al. Serotypes and patterns of antibiotic resistance in strains causing invasive pneumococcal disease in children less than 5 years of age[J]. PLoS ONE, 2013, 8(1): e54254. |