 2016, Vol. 18
2016, Vol. 18

 , 余章斌, 张俊, 陈小慧, 吴薇敏, 楚雪, 刘蓓蓓
, 余章斌, 张俊, 陈小慧, 吴薇敏, 楚雪, 刘蓓蓓 母乳是新生儿肠内营养的首选,对于NICU中早产儿及危重儿来说,母乳喂养不仅有促生长、促成熟和保护作用[1],同时还具有减少肠道喂养不耐受[2-3],减少迟发型败血症[4],减少新生儿坏死性小肠结肠炎[5-6],预防早产儿视网膜病[7-9],促进神经系统发育[10-11],促进脑白质发育[12]等应用价值。国内一项多中心研究表明我国NICU中开展早产儿母乳喂养的单位不到10%[13]。我院于2013年8月1日成立国内第二家、华东地区首家母乳库,极超低出生体重儿住院期间母乳喂养率可达100%,以捐献母乳为主[14]。但捐献母乳多为足月产产妇生后数月后捐赠的,生物活性分子的含量较低,营养成分波动范围大。早产母亲的母乳中蛋白质含量比足月产母亲高,更适合早产儿的需要[15]。如何提高NICU亲母母乳喂养率是我院迫切需要解决的问题。近年来,质量改进(quality improvement)在临床工作中广泛使用[16],其在NICU中的实际应用证明了其对新生儿健康的重要性[17-21],目前国内尚无有关极低和超低出生体重儿母乳质量改进的报道。因此本研究拟就母乳质量改进前后亲母母乳喂养及相关并发症发生情况进行比较,旨在提高NICU中极低和超低出生体重儿的亲母母乳喂养率。
1 资料与方法 1.1 研究对象2014年7月至2016年6月本院收治的极低和超低出生体重儿。所有患儿均系亲母母乳加捐献母乳喂养,优选亲母母乳,亲母母乳不能供给时选择捐献母乳,优选新鲜母乳,新鲜母乳不能满足时给予冻存母乳。
排除标准:(1)孕母有严重疾病、传染性疾病或者其他明确母乳喂养医学禁忌症;(2)早产儿未存活。
1.2 研究方法回顾性调查收集2014年7月至2015年7月本院收治的极低和超低出生体重儿(质量改进前组)以及实施母乳质量改进措施后的2015年8月至2016年6月的极低和超低出生体重儿(质量改进后组)资料。对两组患儿住院期间亲母母乳喂养率、患儿体重增长、首次亲母母乳喂养时间,母乳强化剂添加时间,开始喂养时龄,静脉营养持续时间,达到全肠道喂养的时间,喂养不耐受发生率进行比较。
1.3 相关研究指标的定义亲母母乳喂养率:亲母母乳摄入量占亲母母乳和捐献母乳总摄入量的比率。
喂养不耐受:胃潴留量>喂养量的50%,伴腹胀和(或) 呕吐,并影响肠内喂养方案实施[22]。
全肠道喂养:奶量达每天150 mL/kg。如病程中有禁食情况,则记录第一次达到全肠道喂养时间。
加奶速度:改进前后两组加奶速度相同,均采用本科室不同出生体重极、超低出生体重儿喂养指南[23]进行加奶。见表 1。
| 表 1 不同出生体重极、超低出生体重儿的喂养指南 |

1.4 院内母乳质量改进措施
本研究借鉴了发达国家母乳质量改进的专家组建议[24],根据我院的实际情况制定母乳质量改进措施:(1)发放母乳喂养知识手册及宣教:早产儿入院后发放母乳喂养知识手册,并告知母乳喂养好处及母乳收集、储存与运送方法,家长亦可通过微信平台进一步学习母乳喂养相关知识。(2)母亲尽早开始吸乳:鼓励生后1 h内母亲开始挤奶,床旁宣教和指导,帮助母亲挤奶。(3)提供提高母亲吸乳量的方法:提供医院级别吸奶器及挤奶室,定期让妈妈到NICU探视,鼓励母亲每2~3 h挤奶一次,并填写母乳日志。(4)母乳口腔护理:从早产儿出生可获得亲母母乳开始,应用初乳涂抹于早产儿的口腔,每6 h 1次。(5)NICU袋鼠式护理:无创呼吸支持的患儿均可间断进行袋鼠护理,进行皮肤-皮肤接触,每周1次以上,每次1 h以上。(6)奶嘴、乳房的非营养性吸吮:禁食或不能经口喂养的患儿,鼻饲喂养前给予安抚奶嘴吸吮3~5 min。(7)母乳的管理:亲母母乳运送至母乳库时,在核对信息、奶量后冷藏或冷冻储存。(8)捐赠奶、母乳强化剂规范使用:优选亲母母乳,亲母母乳不能供给时选择捐献母乳。优选新鲜母乳,新鲜母乳不能满足时给予冻存母乳。奶量达每日80~100 mL/kg时添加母乳强化剂。(9)以家庭为中心的家庭化病房:允许患儿父母进入NICU或转入以家庭为中心的陪护病房,教家长为患儿提供部分护理操作,如喂奶,换尿布等。学习喂养与护理,为出院做准备。(10)出院前母乳喂养的再宣教:告知按需喂养及如何增加奶量及母乳强化剂,设立母乳喂养门诊咨询。10项改进措施均是改进后组规范有序的实施。虽然改进前部分措施也偶可实施,但未纳入医嘱,未进行宣教。
1.5 统计分析采用SPSS(22.0)统计分析数据。正态分布的计量资料以均数±标准差(x±s)表示,组间比较采用两独立样本的t检验;计数资料采用率(%)表示,组间比较采用χ2检验。不符合正态分布计量资料以中位数(四分位间距)[M(P25,P75)]表示,组间比较采用独立样本非参数检验,P<0.05为差异有统计学意义。
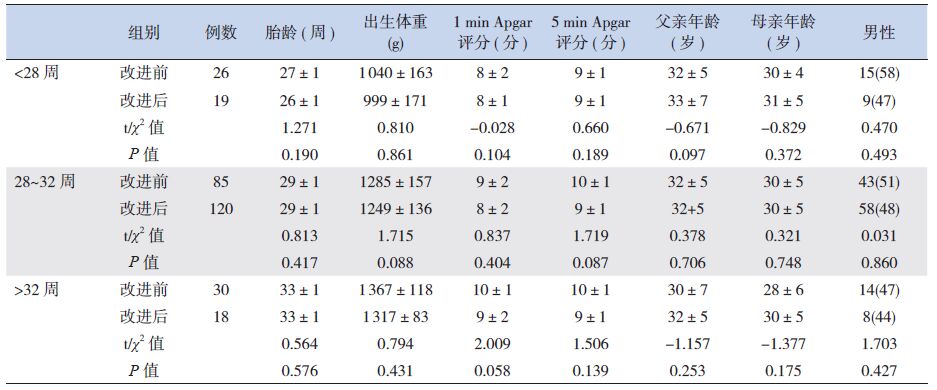
2 结果 2.1 两组一般资料比较质量改进前组患儿141例,其中男性72例,女性69例;胎龄25周~37周,平均胎龄29.6±2.4周;体重750 g~1 490 g,平均1 246±184 g。质量改进后组纳入患儿157例,其中男性75例,女性82例;胎龄25周~35周,平均胎龄29.2±1.8周;体重700 g~1 480 g,平均1 223±163 g。两组患儿的出生胎龄及出生体重、性别、Apgar评分、父母年龄等的差异均无统计学意义。见表 2。
| 表 2 两组一般资料比较 [(x±s)或n(%)] |
2.2 两组患儿住院期间亲母母乳喂养情况
实施质量改进后,亲母母乳喂养量、亲母母乳喂养率均明显增高,捐献母乳喂养量和捐献母乳喂养率均明显降低,差异有统计学意义。见表 3、4。
| 表 3 住院期间两组亲母母乳喂养情况比较 [(x±s)或M(P25,P75)] |

| 表 4 住院期间两组捐献母乳喂养情况比较 [(x±s)或M(P25,P75)] |

2.3 两组患儿住院期间体重增长情况
实施母乳质量改进措施后,7 d时体重仍呈负增长,但母乳质量改进后体重丢失量较改进前减少,14 d时体重上升,母乳质量改进后体重增长速度较改进前快。但出院时两组体重增长速度差异无统计学意义。见表 5。
| 表 5 两组患儿住院期间体重增长情况 [M(P25,P75)] |

2.4 两组患儿住院期间情况的比较
实施母乳质量改进措施后,母乳强化剂添加时间较改进前提前,静脉营养时间较改进前缩短,达全肠道喂养时间较改进前提前,喂养不耐受的发生率较改进前有所改善,差异有统计学意义。开始喂养的时龄及首次亲母母乳喂养的时间差异无统计学意义。见表 6。
| 表 6 不同胎龄患儿在改进前后情况的比较 [n(%)或M(P25,P75)] |

3 讨论
本研究发现实施母乳质量改进后,NICU中极低和超低出生体重儿亲母母乳喂养率可显著提升。国外也有类似报道,如美国某项研究实施母乳质量改进,将其干预措施分为强烈推荐措施(如培训和支持母乳喂养的技巧;建立和掌握稳定的母乳喂养策略,包括尽早挤奶、口腔护理、泵奶日志、专家解答疑惑等等措施;建立稳定的早产儿营养管理措施)和推荐措施(应用标准化的喂养措施,应用如袋鼠护理、非营养性吸吮促进向直接哺乳的转变),成功提高了母乳喂养率[25]。挪威的一项研究通过鼓励、指导提供医院用吸乳器等一系列措施,结合母乳喂养环(一种记录护理操作的环状表格)来记录、追踪亲母乳喂养质量改进实施过程,发现大部分极早产儿母亲也可为其新生儿提供亲母母乳[26]。英国的一项研究,通过实施一系列质量改进护理措施,将纯亲母母乳喂养率从26%提高到33%,将部分亲母母乳喂养率(混合喂养)由50% 提高到57%[27]。本研究实施母乳质量改进措施后,住院期间亲母母乳喂养率也明显增高,与文献相一致。美国的一项研究发现母乳质量改进后,出生14 d内接受母乳达500 ml/kg的极低出生体重儿数量由原来的50%上升到80%[28]。国内胡艳玲等[29]研究发现经质量改进将母乳喂养率从改进前的<1%提升到42%。本研究也发现母乳质量改进措施实施后0~14 d亲母母乳喂养量也有明显上升。
本研究发现母乳质量改进后,极低和超低出生体重儿体重的增长速度较改进前增快,考虑可能与亲母母乳喂养量增多有关。有研究以亲母母乳和/或足月儿母亲的捐献母乳喂养胎龄小于32周的早产儿,发现接受超过80%亲母母乳的孩子比不足20%亲母母乳的孩子体重增长速率更快,且体重增长与摄入亲母母乳的量正相关[30]。同样,在一项回顾性的队列研究中,亲母母乳喂养量超过75%的早产儿与捐献母乳喂养量超过75%的早产儿相比,出院体重位于相同胎龄第十百分位数以下的比率更低[31]。
本研究通过母乳质量改进措施的实施,亲母母乳喂养率显著提升,母乳强化剂添加时间较改进前提前,静脉营养时间较改进前缩短,达全肠道喂养时间较改进前提前,喂养不耐受的发生率较改进前有所改善。这可能与亲母母乳喂养后,肠道益生菌的产生有关。母乳中包含可定植于新生儿肠道的活菌。母乳中的优势菌群是葡萄球菌、链球菌、双歧杆菌、乳酸菌,用吸奶器获得的母乳样本具有更高的细菌总数和肠杆菌比例[32]。而早期的亲母母乳口腔护理可以使母乳中的细胞因子被口腔的颊黏膜吸收而促进免疫系统的发育[33]。也有证据表明,肠道细菌可通过一个内源性途径由单核细胞从肠腔运输至乳腺[34],即肠道共生细菌除了直接的粪口传播之外,还可能通过肠道-乳腺通路垂直传播[35]。肠道-乳腺通路对婴儿粪便中的乳酸杆菌含量可能有更深刻的影响[36]。
综上,亲母母乳对NICU中的极超低出生体重儿来说具有显著的优点。作为国内NICU极低和超低出生体重儿母乳喂养质量改善的起始项目,本课题的经验将对今后针对其他各地区NICU早产儿母乳喂养质量改善,提高早产儿生存质量具有重要的参考价值。
| [1] | Rodríguez JM. The origin of human milk bacteria: is there a bacterial entero-mammary pathway during late pregnancy and lactation?[J]. Adv Nutr , 2014, 5 (6) : 779–784. DOI:10.3945/an.114.007229 |
| [2] | Fanaro S. Feeding intolerance in the preterm infant[J]. Early Hum Dev , 2013, 89 (Suppl 2) : S13–S20. |
| [3] | Sisk PM, Lovelady CA, Gruber KJ, et al. Human milk consumption and full enteral feeding among infants who weigh ≤ 1250 grams[J]. Pediatrics , 2008, 121 (6) : e1528–e1533. DOI:10.1542/peds.2007-2110 |
| [4] | Patel AL, Johnson TJ, Engstrom JL, et al. Impact of early human milk on sepsis and health-care costs in very low birth weight infants[J]. J Perinatol , 2013, 33 (7) : 514–519. DOI:10.1038/jp.2013.2 |
| [5] | Herrmann K, Carroll K. An exclusively human milk diet reduces necrotizing enterocolitis[J]. Breastfeed Med , 2014, 9 (4) : 184–190. DOI:10.1089/bfm.2013.0121 |
| [6] | Johnson TJ, Patel AL, Bigger HR, et al. Cost savings of human milk as a strategy to reduce the incidence of necrotizing enterocolitis in very low birth weight infants[J]. Neonatology , 2015, 107 (4) : 271–276. DOI:10.1159/000370058 |
| [7] | Zhou J, Shukla VV, John D, et al. Human Milk Feeding as a Protective Factor for Retinopathy of Prematurity: A Metaanalysis[J]. Pediatrics , 2015, 136 (6) : e1576–e1586. DOI:10.1542/peds.2015-2372 |
| [8] | Sisk PM, Lovelady CA, Dillard RG, et al. Lactation counseling for mothers of very low birth weight infants: effect on maternal anxiety and infant intake of human milk[J]. Pediatrics , 2006, 117 (1) : e67–e75. DOI:10.1542/peds.2005-0267 |
| [9] | Okamoto T, Shirai M, Kokubo M, et al. Human milk reduces the risk of retinal detachment in extremely low-birthweight infants[J]. Pediatr Int , 2007, 49 (6) : 894–897. DOI:10.1111/ped.2007.49.issue-6 |
| [10] | Rozé JC, Darmaun D, Boquien CY, et al. The apparent breastfeeding paradox in very preterm infants: relationship between breast feeding, early weight gain and neurodevelopment based on results from two cohorts, EPIPAGE and LIFT[J]. BMJ Open , 2012, 2 (2) : e000834. DOI:10.1136/bmjopen-2012-000834 |
| [11] | Meier PP, Engstrom JL, Patel AL, et al. Improving the use of human milk during and after the NICU stay[J]. Clin Perinatol , 2010, 37 (1) : 217–245. DOI:10.1016/j.clp.2010.01.013 |
| [12] | Deoni SC, Dean DC 3rd, Piryatinsky I, et al. Breastfeeding and early white matter development: A cross-sectional study[J]. Neuroimage , 2013, 82 : 77–86. DOI:10.1016/j.neuroimage.2013.05.090 |
| [13] | 中国医师协会新生儿专业委员会-营养专家委员会协作组. 极低出生体质量早产儿院内营养现状多中心调查[J]. 临床儿 科杂志 , 2015, 33 (1) : 32–37. |
| [14] | 韩树萍, 余章斌. 母乳库建立和运行管理的相关指南解读[J]. 中华围产医学杂志 , 2014, 17 (7) : 433–437. |
| [15] | 何必子, 孙秀静, 全美盈, 等. 早产母乳营养成分的分析[J]. 中国当代儿科杂志 , 2014, 16 (7) : 679–683. |
| [16] | 张俊, 刘凤, 韩树萍. NICU 母乳喂养质量改进进展[J]. 临床 儿科杂志 , 2016, 34 (1) : 74–77. |
| [17] | Lee SK, Aziz K, Singhal N, et al. Improving the quality of care for infants: a cluster randomized controlled trial[J]. CMAJ , 2009, 181 (8) : 469–476. DOI:10.1503/cmaj.081727 |
| [18] | Mola SJ, Annibale DJ, Wagner CL, et al. NICU bedside caregivers sustain process improvement and decrease incidence of bronchopulmonary dysplasia in infants <30 weeks gestation[J]. Respir Care , 2015, 60 (3) : 309–320. DOI:10.4187/respcare.03235 |
| [19] | Lee SK, Shah PS, Singhal N, et al. Association of a quality improvement program with neonatal outcomes in extremely preterm infants: a prospective cohort study[J]. CMAJ , 2014, 186 (13) : e485–e494. DOI:10.1503/cmaj.140399 |
| [20] | Wellington A, Perlman JM. Infant-driven feeding in premature infants: a quality improvement project[J]. Arch Dis Child Fetal Neonatal Ed , 2015, 100 (6) : F495–F500. DOI:10.1136/archdischild-2015-308296 |
| [21] | Lu PL, Teich S, Di Lorenzo C, et al. Improvement of quality of life and symptoms after gastric electrical stimulation in children with functional dyspepsia[J]. Neurogastroenterol Motil , 2013, 25 (7) : 567–e456. DOI:10.1111/nmo.12104 |
| [22] | 曹云. 早产儿喂养不耐受及处理策略[J]. 中国新生儿科杂志 , 2015, 30 (3) : 169–171. |
| [23] | Dutta S, Singh B, Chessell L, et al. Guidelines for feeding very low birth weight infants[J]. Nutrients , 2015, 7 (1) : 423–442. DOI:10.3390/nu7010423 |
| [24] | Nyqvist KH, Häggkvist AP, Hansen MN, et al. Expansion of the baby-friendly hospital initiative ten steps to successful breastfeeding into neonatal intensive care: expert group recommendations[J]. J Hum Lact , 2013, 29 (3) : 300–309. DOI:10.1177/0890334413489775 |
| [25] | Lee HC, Kurtin PS, Wight NE, et al. A quality improvement project to increase breast milk use in very low birth weight infants[J]. Pediatrics , 2012, 130 (6) : e1679–e1687. DOI:10.1542/peds.2012-0547 |
| [26] | Husebye ES, Kleven IA, Kroken LK, et al. See the search details. Targeted program for provision of mother's own milk to very low birth weight infants[J]. Pediatrics , 2014, 134 (2) : e489–e495. DOI:10.1542/peds.2013-2463 |
| [27] | Battersby C, Santhakumaran S, Upton M, et al. The impact of a regional care bundle on maternal breast milk use in preterm infants: outcomes of the East of England quality improvement programme[J]. Arch Dis Child Fetal Neonatal Ed , 2014, 99 (5) : F395–F401. DOI:10.1136/archdischild-2013-305475 |
| [28] | Ward L, Auer C, Smith C, et al. The human milk project: a quality improvement initiative to increase human milk consumption in very low birth weight infants[J]. Breastfeed Med , 2012, 7 : 234–240. DOI:10.1089/bfm.2012.0002 |
| [29] | 胡艳玲, 万兴丽, 苏绍玉. 应用PDCA 持续提高新生儿母婴 分离时的母乳喂养率[J]. 中国实用护理杂志 , 2014, 30 (z2) : 82–83. |
| [30] | Montjaux-Régis N, Cristini C, Arnaud C, et al. Improved growth of preterm infants receiving mother's own raw milk compared with pasteurized donor milk[J]. Acta Paediatr , 2011, 100 (12) : 1548–1554. DOI:10.1111/j.1651-2227.2011.02389.x |
| [31] | Colaizy TT, Carlson S, Saftlas AF, et al. Growth in VLBW infants fed predominantly fortified maternal and donor human milk diets: a retrospective cohort study[J]. BMC Pediatr , 2012, 12 : 124. DOI:10.1186/1471-2431-12-124 |
| [32] | Marín ML, Arroyo R, Jiménez E, et al. Cold storage of human milk: effect on its bacterial composition[J]. J Pediatr Gastroenterol Nutr , 2009, 49 (3) : 343–348. DOI:10.1097/MPG.0b013e31818cf53d |
| [33] | Rodriguez NA, Meier PP, Groer MW, et al. Oropharyngeal administration of colostrum to extremely low birth weight infants: theoretical perspectives[J]. J Perinatol , 2009, 29 (1) : 1–7. DOI:10.1038/jp.2008.130 |
| [34] | Perez PF, Doré J, Leclerc M, et al. Bacterial imprinting of the neonatal immune system: lessons from maternal cells?[J]. Pediatrics , 2007, 119 (3) : e724–e732. DOI:10.1542/peds.2006-1649 |
| [35] | Albesharat R, Ehrmann MA, Korakli M, et al. Phenotypic and genotypic analyses of lactic acid bacteria in local fermented food, breast milk and faeces of mothers and their babies[J]. Syst Appl Microbiol , 2011, 34 (2) : 148–155. DOI:10.1016/j.syapm.2010.12.001 |
| [36] | Martín R, Heilig HG, Zoetendal EG, et al. Cultivationindependent assessment of the bacterial diversity of breast milk among healthy women[J]. Res Microbiol , 2007, 158 (1) : 31–37. DOI:10.1016/j.resmic.2006.11.004 |