 2016, Vol. 18
2016, Vol. 18

 , 刘丽梅1, 谷容1, 赵晓东1
, 刘丽梅1, 谷容1, 赵晓东1 2. 重庆医科大学药学院临床药学教研室, 重庆 400016
据2014年哮喘流行病学调查显示,中国约有2 000万人罹患哮喘[1];国外研究发现在发达国家哮喘的发病率在过去30年里翻了一番[2]。哮喘是儿童常见的慢性肺部疾病,不仅严重影响了患者的生活质量,而且造成了巨大的个人和社会经济负担,因此如何防治哮喘已成为医学界所面临的重要课题。然而哮喘发病及加重的影响因素众多,近年来基于“卫生假说——生命早期抗菌药物使用与儿童哮喘之间存在因果关系”,相继出现许多关于这方面的报道,其中多个回顾性研究[3-6]表明的确存在正相关关系。这些研究均采用国际儿童哮喘与过敏研究(International Study of Asthma and Allergies in Childhood,ISAAC)问卷调查,但仅从患儿或其父母回忆获得的资料多存在回忆偏倚。为了避免回顾性研究的偏倚,研究者们做了大量的前瞻性或纵向研究,但仍有个别研究对其是否正相关存在怀疑态度[7],其中最受争议的问题包括逆向因果和指示混淆,对于逆向因果关系,主要是不能区分抗菌药物使用是在哮喘后发生还是在哮喘前发生;指示混淆是指无法分清就诊次数的增加增加了哮喘的风险还是就诊次数增加从而增加了抗菌药物的使用几率或次数。还有研究报道指出,关于儿童时期的哮喘,或许我们并不能把他看成是某单一因素造成的,而是多种因素共同造成的[8];也有研究表明抗菌药物的种类和使用频次对研究结果造成影响[9]。
本研究拟通过全面收集生命早期使用抗菌药物与儿童哮喘的相关性的前瞻性队列研究,系统性评价出生后1年内使用抗菌药物与儿童哮喘的关系,包括抗菌药物的使用频次及高风险人群抗生素的使用与儿童时期的哮喘的关系,以期健全抗菌药物的合理应用。
1 资料与方法 1.1 文献纳入标准(1)研究类型:前瞻性队列研究,病例数目不限。(2)研究对象:出生后1年内至少使用过1次抗菌药物的婴儿。(3)暴露因素:暴露组为出生后1年内使用抗菌药物的婴儿,对照组为出生后1年内没有使用过抗菌药物的婴儿。(4)结局指标:2~12岁期间被诊断为哮喘。
1.2 文献排除标准(1)非队列研究。(2)随访<1年的研究。 (3)数据不全或无法获取数据的文献。(4)仅有摘要的会议汇编。(5)重复发表或资料雷同的研究只保留其中质量较高的一个。(6)排除局部抗菌药物使用的文献。
1.3 文献检索策略文献检索的中文数据库为中国知网数据库、中国维普科技期刊数据库和万方数据库。中文主题词包括新生儿、婴幼儿、儿童、学龄前儿童;哮喘、支气管哮喘、变异性哮喘;抗菌药物、抗生素。文献检索的外文数据库为PubMed和EBSCO,英文检索词包括:asthma,allergic disease,bronchial asthma,allergic asthma,anti-bacterial agents,anti-infective agents,antimicrobial,antibacterial,antibiotic,newborn,infant,neonat*,childhood,preschool children,early life。检索时间均从1999年至2016年4月。
1.4 文献筛选及资料提取由2位评价者按照统一的表格独立地对文献的一般资料、干预措施,包括抗菌药物的使用类别、疗程、调整因素及诊断哮喘时的年龄等资料进行提取,并进行交叉核对。出现分歧时通过讨论,必要时由第3位人员协助解决。资料提取中:对于同时存在其他过敏性疾病,如花粉过敏、湿疹、特应性皮炎的研究,只使用其中关于哮喘的风险评估;对于同时存在其他药物如布洛芬和对乙酰氨基酚的使用与哮喘的关系的研究,只使用其中抗菌药物与哮喘的关系的数据;对于年龄范围较大,选择提取出本文设定的年龄范围的数据。
1.5 纳入文献的质量评价标准按照Cochrane系统评价员手册5. 0. 1推荐的队列研究的偏倚风险评价方法:纽卡斯尔-渥太华量表(The Newcastle-Ottawa Scale,NOS)[10]。通过对人群选择、组间可比性、暴露因素测量对文献质量进行评价,满分为9分,纳入文献要求组间可比性板块满分(2分),总分≥6分为质量高的研究。两名研究者独立完成质量评价,若有分歧则通过讨论、请教专家或参考第三位评价者的建议决定是否纳入。
1.6 统计学分析进入Meta分析的效应量为各研究调整后的效应值(HR、RR、OR)及其95%CI。通过Cochran's χ2检验为基础的Q检验和I2检验,检验其异质性,若P>0.1和I2<50%,提示无统计学异质性,采用固定效应模型分析;若存在统计学异质性(P≤0.1,I2≥50%)时,采用随机效应模型分析。最后使用Begg's及Egger's检验定量评估发表偏倚。计数资料统计量采用RR、OR、HR及其95%CI表示。P<0.05为差异有统计学意义。以上所有分析均使用Stata12.0进行分析。
1.7 敏感性分析将纳入的每个研究依次排除后,观察总的效应值的变化情况,以检验整个研究的稳定性。
2 结果 2.1 文献检索及纳入情况经上述检索策略检索文献1 274篇,经Endnote软件及手工除重、阅读文献题目及摘要排除没有评估抗菌药物的使用与哮喘关系的文献后保留文献60篇;全文阅读后排除横断面研究、回顾性队列研究、巢式病例对照、病例对照、干预因素不符合、研究对象不符合、结局指标不符合的文献,最后纳入研究14项。
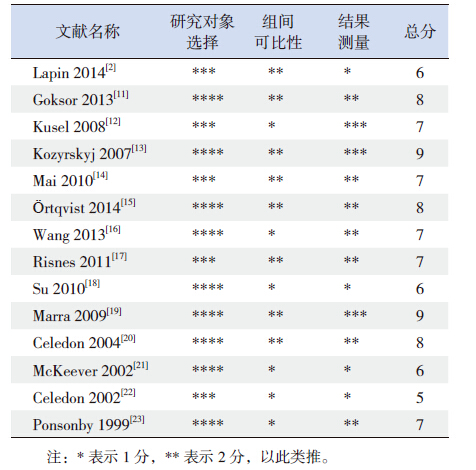
按照NOS评价方法,对所纳入的14项研究进行评价(表 1),其中13项属于高质量研究(总分≥6分)。14项研究均属于前瞻性队列研究,并且都调整了混杂因素,包括了从1999~2014年的研究,样本量198~493 785人。其中有3项研究的研究对象是至少有1位亲属有过敏性疾病的高风险人群,样本量为946人,诊断哮喘140人;有4项研究其暴露因素是使用抗菌药物分别在出生后的1周、3个月、6个月和9个月;有1项研究队列样本量3 306人,对4岁和8岁诊断哮喘的患儿做了统计,其中4岁年龄段的125人,8岁年龄段的104人;余下的6项研究样本量有1 057 662人,诊断哮喘的有113 283人,其中1项研究对两个独立的出生队列做了观察。
| 表 1 纳入研究的方法学质量评价 |
2.2 Meta分析结果 2.2.1 出生后1年内使用抗菌药物与儿童哮喘的关系
对14项研究的结果进行数据合并后,异质性检验显示I2=86.7%,P<0.001,故采用随机效应模型分析结果,其合并效应量为OR=1.31,95%CI:1.18~1.46,提示出生后1年内使用抗菌药物增加儿童时期哮喘的风险(图 1)。

|
图 1 1 岁以内儿童使用抗菌药物后儿童时期患哮喘风 险的Meta 分析 |
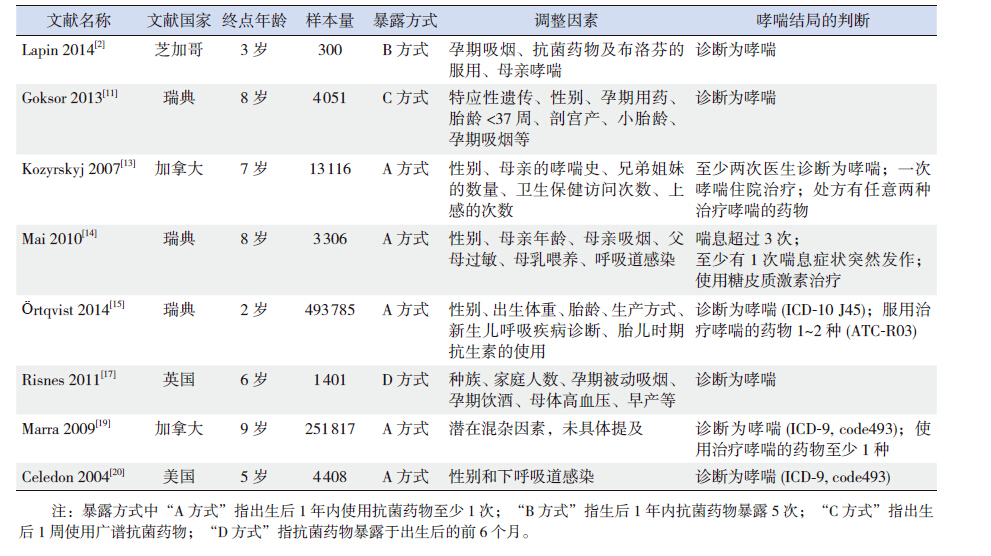
但由于上述所纳入研究异质性大,选取其中质量高、且调整下呼吸道感染的混淆因素后的8项研究(表 2)再次分析,异质性检验显示异质性小(I2=41.0%,P=0.105),使用固定效应模型分析,OR=1.14,95%CI:1.10~1.17,P<0.05,提示在调整下呼吸道感染的混淆因素后,出生后1年内使用抗菌药物对儿童时期哮喘的风险仍有所增加(图 2)。
| 表 2 调整了下呼吸道感染因素后的8 项研究 |

|
图 2 调整下呼吸道感染后罹患哮喘风险的Meta 分析 |
2.2.2 出生后1年内使用抗菌药物>4次与儿童哮喘的关系
纳入通过文献质量评分质量较高的研究,合并出生后1年内使用抗菌药物>4次的效应量,共4篇。使用固定效应模型进行分析(I2=27.3%,P=0.248),显示OR =1.28,95%CI:1.19~1.38,P<0.05(图 3),提示出生后1年内使用抗菌药物超过4次的哮喘风险是使用0~1次的1.28倍。

|
图 3 1 岁以内使用>4 次抗菌药物后患哮喘风险的 Meta 分析 |
2.2.3 出生后1年内使用抗菌药物与儿童哮喘的关系(高风险人群)
对其中3项研究对象是至少有1位亲属有过敏性疾病的高风险人群的结果进行合并,通过固定效应模型分析(I2=38.8%,P=0.195),显示OR =1.47,95%CI:1.20~1.81,P<0.05(图 4),提示至少有1位亲属患有过敏性疾病的高风险儿童,在其出生后1年内使用抗菌药物患哮喘的风险是其他儿童的1.47倍。

|
图 4 高风险儿童1 岁以内使用抗菌药物后患哮喘风 险的Meta 分析 |
2.2.4 发表偏倚
采用Begg's和Egger's检验对以上纳入的8项质量较高且调整了下呼吸道感染影响因素的研究进行发表偏倚检验,Begg's 检验示P值为0.035;Egger's 检验示P值为0.154,提示不存在任何发表偏倚。
2.2.5 敏感性分析将纳入的8项质量较高且调整了下呼吸道感染影响因素的研究进行敏感性分析,由图 5可知,Marra 等[19]研究可能对结果有较大的影响,去除该研究后,结果为OR =1.24,95%CI:1.14~1.36,P<0.05,并未对最终结果造成影响。

|
图 5 纳入文献的敏感性分析 |
3 讨论
本Meta分析结果表明,在调整下呼吸道感染后,出生后1年内使用抗菌药物其随后在儿童时期的哮喘风险是未使用抗菌药物的1.14倍。由于下呼吸道感染与哮喘的前期症状不能完全分开,影响了抗菌药物的使用与哮喘关系的判断,容易导致逆因果关系的出现(认为患儿在患有下呼吸道感染并使用抗菌药物治疗前其实患儿已患有哮喘),因此对下呼吸道感染进行调控是十分有必要的。控制下呼吸道感染这一混杂因素的方法是未来研究的重要方面。本Meta分析对下呼吸道感染进行了调控,儿童时期罹患哮喘的风险依然增加,说明生后1岁以内抗菌药物的使用的确增加了儿童时期罹患哮喘的风险。
本Meta分析显示,在至少有1位直系亲属有哮喘史的高风险人群中,出生后1年内使用抗菌药物的哮喘风险是未使用的1.47倍,表明具有哮喘家族史的儿童,在生命早期使用抗菌药物后儿童时期罹患哮喘的风险更大。
另外,本Meta分析还显示,出生后1年内使用抗菌药物超过4次者罹患哮喘的风险是使用0~1次的1.28倍,可以得出生命早期抗菌药物的使用次数增加会导致儿童时期罹患哮喘的风险增加,但其中具体的剂量关系、使用疗程的长短,使用抗菌药物的类型均有待进一步研究。
本研究的局限性包括:(1)所纳入的研究人群主要为欧洲人和美洲人,这使得结果的外推性受到影响,因种族的差异,结论不一定适应于其他国家和地区的人群。(2)虽然Meta分析结果显示抗菌药物使用次数>4次时哮喘风险与使用0~1次相比增加了,但并不能得出具体的剂量关系。
(3)2015 GINA全球哮喘处理和预防策略指南[24]指出≤5岁儿童确诊为哮喘是困难的,但本研究结局指标年龄设在2~12岁,在纳入的8篇研究中3篇研究[2, 15, 20]的结局年龄≤5岁,考虑文中明确指出哮喘的诊断结果,故纳入,但不可否认≤5岁儿童诊断哮喘仍存在困难。(4)纳入的各项研究其抗菌药物类别设定是不同的,包括广谱抗菌药物、窄谱抗菌药物的分类或者是青霉素类、头孢菌素类、磺胺类、大环内酯类,故而无法得出哮喘风险的增加与各类抗菌药物的关系。
综上所述,1岁以内抗生素的使用可增加儿童时期罹患哮喘的风险;有1位直系亲属曾患哮喘的儿童1岁内使用抗菌药物罹患哮喘的风险增加;生后1年内抗生素使用次数的增加与哮喘风险的增加有关,但具体的剂量关系有待进一步研究。
| [1] | 冯晓凯. 我国支气管哮喘患病情况及相关危险因素的流行病 学调查[D]. 北京: 北京协和医学院, 2014. |
| [2] | Lapin B, Piorkowski J, Ownby D, et al. The relationship of early-life antibiotic use with asthma in at-risk children[J]. J Allergy Clin Immunol , 2014, 134 (3) : 728–729. DOI:10.1016/j.jaci.2014.05.006 |
| [3] | Metsala J, Lundqvist A, Virtao LJ, et al. Prenatal and post-natal exposure to antibiotics and risk of asthma in childhood[J]. Clin Exp Allergy , 2015, 45 (1) : 137–145. DOI:10.1111/cea.2014.45.issue-1 |
| [4] | Raciborski F, Tomaszewska A, Komorowski J, et al. The relationship between antibiotic therapy in early childhood and the symptoms of allergy in children aged 6–8 years—the questionnaire study results[J]. Int J Occup Med Environ Health , 2012, 25 (4) : 470–480. |
| [5] | Ong MS, Umetsu DT, Mandl KD. Consequences of antibiotics and infections in infancy: bugs, drugs, and wheezing[J]. Ann Allergy Asthma Immunol , 2014, 112 (5) : 441–445. DOI:10.1016/j.anai.2014.01.022 |
| [6] | Cullinan P, Harris J, Mills P, et al. Early prescriptions of antibiotics and the risk of allergic disease in adults: a cohort study[J]. Thorax , 2004, 59 (1) : 11–15. |
| [7] | Kuo CH, Kuo HF, Huang CH, et al. Early life exposure to antibiotics and the risk of childhood allergic diseases: an update from the perspective of the hygiene hypothesis[J]. J Microbiol Immunol Infect , 2013, 46 (5) : 320–329. DOI:10.1016/j.jmii.2013.04.005 |
| [8] | Semic-Jusufagic A, Belgrave D, Pickles A, et al. Assessing the association of early life antibiotic prescription with asthma exacerbations, impaired antiviral immunity, and genetic variants in 17q21: a population-based birth cohort study[J]. Lancet Respir Med , 2014, 2 (8) : 621–630. DOI:10.1016/S2213-2600(14)70096-7 |
| [9] | Marra F, Marra CA, Richardson K, et al. Antibiotic consumption in children prior to diagnosis of asthma[J]. BMC Pulm Med , 2011, 11 : 32. DOI:10.1186/1471-2466-11-32 |
| [10] | Wells GA, Shea B, Connell DO, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses[J]. Appl Eng Agric , 2002, 18 (6) : 727–734. |
| [11] | Goksor E, Alm B, Pettersson R, et al. Early fish introduction and neonatal antibiotics affect the risk of asthma into school age[J]. Pediatr Allergy Immunol , 2013, 24 (4) : 339–344. DOI:10.1111/pai.2013.24.issue-4 |
| [12] | Kusel MM, De Klerk N, Holt PG, et al. Antibiotic use in the first year of life and risk of atopic disease in early childhood[J]. Clin Exp Allergy , 2008, 38 (12) : 1921–1928. DOI:10.1111/cea.2008.38.issue-12 |
| [13] | Kozyrskyj AL, Ernst P, Becker AB. Increased risk of childhood asthma from antibiotic use in early life[J]. Chest , 2007, 131 (6) : 1753–1759. DOI:10.1378/chest.06-3008 |
| [14] | Mai XM, Kull I, Wickman M, et al. Antibiotic use in early life and development of allergic diseases: respiratory infection as the explanation[J]. Clin Exp Allergy , 2010, 40 (8) : 1230–1237. DOI:10.1111/j.1365-2222.2010.03532.x |
| [15] | Örtqvist AK, Lundholm C, Kieler H, et al. Antibiotics in fetal and early life and subsequent childhood asthma: nationwide population based study with sibling analysis[J]. BMJ , 2014, 349 : g6979. |
| [16] | Wang JY, Liu LF, Chen CY, et al. Acetaminophen and/or antibiotic use in early life and the development of childhood allergic diseases[J]. Int J Epidemiol , 2013, 42 (4) : 1087–1099. DOI:10.1093/ije/dyt121 |
| [17] | Risnes KR, Belanger K, Murk W, et al. Antibiotic exposure by 6 months and asthma and allergy at 6 years: findings in a cohort of 1,401 US children[J]. Am J Epidemiol , 2011, 173 (3) : 310–318. DOI:10.1093/aje/kwq400 |
| [18] | Su Y, Rothers J, Stern DA, et al. Relation of early antibiotic use to childhood asthma: confounding by indication?[J]. Clin Exp Allergy , 2010, 40 (8) : 1222–1229. DOI:10.1111/j.1365-2222.2010.03539.x |
| [19] | Marra F, Marra CA, Richardson K, et al. Antibiotic use in children is associated with increased risk of asthma[J]. Pediatrics , 2009, 123 (3) : 1003–1010. DOI:10.1542/peds.2008-1146 |
| [20] | Celedon JC, Fuhlbrigge A, Rifas-Shiman S, et al. Antibiotic use in the first year of life and asthma in early childhood[J]. Clin Exp Allergy , 2004, 34 (7) : 1011–1016. DOI:10.1111/cea.2004.34.issue-7 |
| [21] | McKeever TM, Lewis SA, Smith C, et al. Early exposure to infections and antibiotics and the incidence of allergic disease: a birth cohort study with the West Midlands General Practice Research Database[J]. J Allergy Clin Immunol , 2002, 109 (1) : 43–50. DOI:10.1067/mai.2002.121016 |
| [22] | Celedon JC, Litonjua AA, Ryan L, et al. Lack of association between antibiotic use in the first year of life and asthma, allergic rhinitis, or eczema at age 5 years[J]. Am J Respir Crit Care Med , 2002, 166 (1) : 72–75. DOI:10.1164/rccm.2109074 |
| [23] | Ponsonby AL, Couper D, Dwyer T, et al. Relationship between early life respiratory illness, family size over time, and the development of asthma and hay fever: a seven year follow up study[J]. Thorax , 1999, 54 (8) : 664–669. DOI:10.1136/thx.54.8.664 |
| [24] | Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention[EB/OL]. (May 2015). www.ginasthma.org. |