 2017, Vol. 19
2017, Vol. 19



小于胎龄儿(small for gestational age, SGA)又称宫内发育迟缓(intrauterine growth retardation, IUGR)儿。有研究发现,SGA在胎儿期肾脏体积明显缩小、肾单位数目明显减少,成年后容易发生心血管、糖尿病等代谢综合征[1-2]。有长期随访研究发现,IUGR增加了终末期肾脏疾病(end-stage renal disease, ESRD)和蛋白尿的发生风险[3-4]。但是目前关于SGA儿生后早期肾脏功能的研究尚少,结论不一。本研究对SGA儿生后早期肾脏功能进行回顾性对照研究,探寻SGA儿早期肾功能损害的诊断方法,以便及时干预,减低未来慢性肾脏病的发生风险。
1 资料与方法 1.1 研究对象选择2013年1月至2015年3月北京大学第三医院新生儿病房的早产SGA儿40例、足月SGA儿33例作为研究对象,均为出生后24 h内收住院。
排除标准:(1)胎龄 < 28周或≥42周;(2)重要脏器先天畸形(心、脑、肾);(3)先天肾脏疾病;(4)双胎输血综合征患者;(5)生后1 min Apgar评分≤7分。
40例早产SGA,按照1:2比例匹配同期住院且出生胎龄相差不超过1周、性别相同的生后24 h内入院的早产适于胎龄儿(appropriate for gestational age, AGA)80人为对照;33例足月SGA,按照1:1比例匹配同期住院且出生胎龄相差不超过1周、性别相同的生后24 h内入院的足月AGA儿33人为对照。
SGA、AGA诊断依据实用新生儿学[5]。
1.2 研究方法回顾性分析、比较SGA、AGA儿的尿素氮(blood urea nitrogen, BUN)、血清肌酐(serum creatinine, SCr)、估算肾小球滤过率(estimate glomerular filtration rate, eGFR)、血压、单位体重尿量以及蛋白尿情况。
收集资料,包括:(1)胎龄、出生体重、出生身长;(2)入院48 h内的BUN、SCr;(3)入院时血压;(4)入院后第1天的24 h尿量(通过尿布称重间接计算尿量);(5)生后1周内的随机尿常规。
根据Schwartz公式[6]计算eGFR。
eGFR=k×身长(cm)/ SCr(mg/dL),早产儿k值为0.33、足月儿为0.45。
1.3 统计学分析所有数据采用SPSS 22.0软件进行统计学处理。使用Kolmogorov-Smirnov检验对各计量资料进行正态性检验。正态分布的计量资料以均数±标准差(x±SD)表示,两组间比较采用t检验;非正态分布的资料采用中位数四分位间距[P50(P25,P75)]描述,两组间比较采用秩和检验(Mann-Whitney U test)。计数资料以百分率表示,两组间的比较采用χ2检验。P < 0.05为差异有统计学意义。
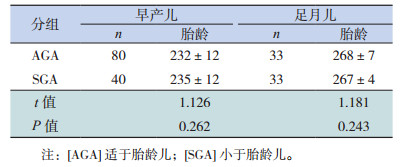
2 结果 2.1 一般资料早产儿AGA与SGA之间,以及足月儿AGA与SGA之间的出生胎龄差异无统计学意义(P > 0.05),见表 1。
| 表 1 AGA、SGA组出生胎龄的比较(x± s,d) |
2.2 SGA和AGA组肾脏功能的比较
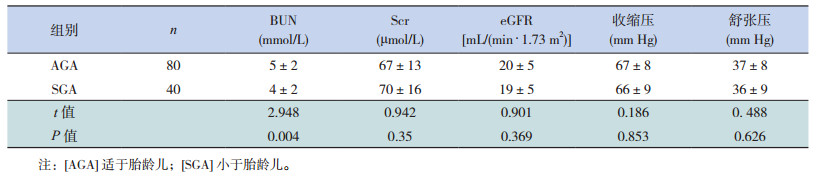
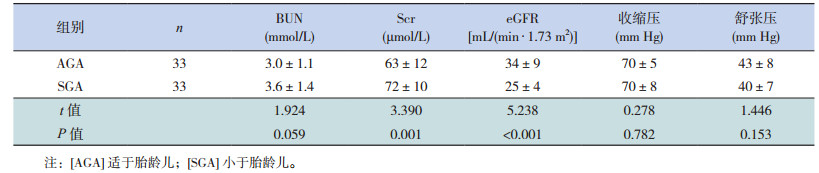
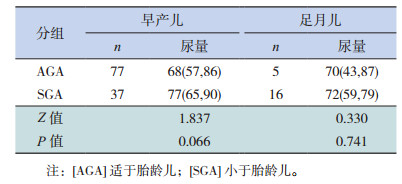
早产儿SGA组的BUN低于AGA组(P=0.004),两组间SCr、eGFR、血压的差异均无统计学意义(P > 0.05),见表 2。足月儿SGA与AGA组BUN、血压的差异无统计学意义(P > 0.05);SGA组的SCr值较高、eGFR较低,差异均有统计学意义(P < 0.05),见表 3。早产儿AGA与SGA之间,以及足月儿AGA与SGA之间单位体重尿量的差异均无统计学意义(P > 0.05),见表 4。早产儿AGA与SGA之间蛋白尿发生率的差异无统计学意义(P > 0.05),见表 5。足月AGA与SGA均无蛋白尿发生。
| 表 2 早产儿AGA与SGA的肾功能及血压比较(x± s) |
| 表 3 足月儿AGA与SGA的肾功能及血压比较(x± s) |
| 表 4 AGA与SGA的单位体重尿量比较[P50(P25, P75),mL/kg] |
| 表 5 早产儿SGA与AGA的蛋白尿发生率比较[例(%)] |

3 讨论
SGA儿肾单位数量减少,在没有高滤过代偿的情况下,其肾小球滤过率(glomerular filtration rate, GFR)低于AGA。本研究早产儿SGA的BUN低于AGA,而足月儿SGA与AGA的BUN差异无统计学意义,提示BUN可能不是反映SGA早期肾小球滤过功能减退的敏感指标。SCr相比BUN而言,受肾小球滤过功能以外因素的影响较少。本研究中,足月儿SGA组的SCr较AGA组增高,而早产儿SGA组与AGA组的SCr差异无统计学意义。早产儿病情相对复杂,影响肾脏功能的因素较多,且SCr水平也可受年龄、性别、肌肉体积、运动和饮食等因素影响;而且部分肌酐从肾小管分泌,导致血肌酐与肾小球滤过率降低不一定相关[7-8]。
Schwartz公式克服了年龄、性别、身高以及肌肉容量对血肌酐的影响,可以更准确地用于GFR评估。本研究足月儿SGA组较AGA组的eGFR减低,早产儿SGA组与AGA组间的差异无统计学意义。提示IUGR可能降低肾小球的滤过功能,而早产儿eGFR可受到更多因素的影响,如生后早期或母亲产前应用的非甾体类抗炎药、抗生素、激素等药物以及生后早期循环不稳定等,因此在今后的研究中应将影响SGA早期肾功能的相关因素进行分层分析。
Bacchetta等[11]对IUGR儿平均随访7.6年,发现IUGR儿幼年时期的GFR(用菊粉清除率估计)仍低于同龄的AGA。因此针对小于胎龄儿的肾功能需进一步延长随访时间、扩大样本量进行研究,以了解IUGR对于远期肾功能的影响。
有研究表明,低出生体重和肾小球数目减少可导致尿微量蛋白增多,进而产生蛋白尿[13]。动物实验证明[3],IUGR大鼠蛋白尿水平明显高于非IUGR组。本研究为回顾性研究,根据尿蛋白定性结果,早产儿AGA与SGA之间蛋白尿发生率的差异无统计学意义,足月儿AGA与SGA组均无蛋白尿发生。但有研究指出,单纯的尿蛋白定性无法客观、全面地反映肾脏功能,而尿微量蛋白的异常对于肾功能损害的诊断具有更好的指导意义[14]。因此,进一步的研究应前瞻性地以尿微量蛋白作为反映肾功能的指标,以更好地指导临床。
尿量在新生儿群体很难准确计量,受肾前性因素影响也较大。本研究早产儿或足月儿的AGA与SGA之间,单位体重尿量差异均无统计学意义,提示单位体重尿量不能作为反映早期肾功能损害的敏感指标。
自Barker等[15]首次报道出生体重与心血管疾病相关,越来越多的证据表明IUGR及低出生体重是成年期发生高血压的危险因素[16-17]。但大多数研究显示,SGA与AGA在儿童时期的血压差异并无统计学意义[18]。Vehaskari等[19]的一项研究显示,生后4周的IUGR大鼠血压与对照组的差异无统计学意义,而生后8周大鼠的收缩压高于对照组,并且血压增高有随年龄增长而加重的趋势。本研究中早产或足月儿SGA与AGA的入院时血压差异均无统计学意义,与IUGR对生后早期血压影响不大这一结论相符,但应进行长期随访以评估其对远期血压的影响。
在新生儿尤其是早产儿中,还存在多种影响肾脏功能的因素,包括新生儿或孕母应用的多种药物,如非甾体类抗炎药、抗生素、血管紧张素受体阻滞剂、硫酸镁、激素等,以及生后肠内、肠外营养等。本研究仅排除严重心、脑、肾疾病、及窒息等影响因素,未针对其他因素进行分层分析,存在不足,在今后的进一步研究中将扩大样本量,并对小于胎龄儿生后早期肾脏功能的影响因素进行分层探讨。
| [1] | Saha K, Shahida SM, Chowdhury NI, et al. Relationship between estimated foetal weight and renal volume in intra uterine growth retarded foetus in Bangladeshi women[J]. Mymensingh Med J, 2014, 23 (4): 752–757. |
| [2] | Mishra K, Datta V, Aarushi A, et al. The association between weight for gestational age and kidney volume:a study in newborns in India[J]. Iran J Pediatr, 2014, 24 (1): 93–99. |
| [3] | Murano Y, Nishizaki N, Endo A, et al. Evaluation of kidney dysfunction and angiotensinogen as an early novel biomarker of intrauterine growth restricted offspring rats[J]. Pediatr Res, 2015, 78 (6): 678–682. DOI:10.1038/pr.2015.153 |
| [4] | Yim HE, Yoo KH. Early life obesity and chronic kidney disease in later life[J]. Pediatr Nephrol, 2015, 30 (8): 1255–1263. DOI:10.1007/s00467-014-2922-4 |
| [5] | 陈超, 金汉珍. 新生儿分类[M]//邵肖梅, 叶鸿瑁, 邱小汕. 实用新生儿科学. 第4版. 北京: 人民卫生出版社, 2011: 46-47. |
| [6] | Schwartz GJ, Brion LP, Spitzer A. The use of plasma creatinine concentration for estimating glomerular filtration rate in infants, children, and adolescents[J]. Pediatr Clin North Am, 1987, 34 (3): 571–590. DOI:10.1016/S0031-3955(16)36251-4 |
| [7] | Perrone RD, Madias NE, Levey AS. Serum creatinine as an index of renal function:new insights into old concepts[J]. Clin Chem, 1992, 38 (10): 1933–1953. |
| [8] | 徐虹. 几种检测肾小球功能的方法及评价[J]. 中国实用儿科杂志, 2003, 18 (8): 449–451. |
| [9] | Schreuder MF, Wilhelm AJ, BökenkampA, et al. Impact of gestational age and birth weight on amikacin clearance on day 1 of life[J]. Clin J Am Soc Nephrol, 2009, 4 (11): 1774–1778. DOI:10.2215/CJN.02230409 |
| [10] | 黄梅, 韦丹. 早产小于胎龄儿早期肾功能动态变化[J]. 检验医学与临床, 2014, 11 (9): 1236–1237. |
| [11] | Bacchetta J, Harambat J, Dubourg L, et al. Both extrauterine and intrauterine growth restriction impair renal function in children born very preterm[J]. Kidney Int, 2009, 76 (4): 445–452. DOI:10.1038/ki.2009.201 |
| [12] | Viazzi F, Leoncini G, Conti N, et al. Microalbuminuria is a predictor of chronic renal insufficiency in patients without diabetes and with hypertension:the MAGIC study[J]. Clin J Am Soc Nephrol, 2010, 5 (6): 1099–1106. DOI:10.2215/CJN.07271009 |
| [13] | Painter RC, Roseboom TJ, van Montfrans GA, et al. Microalbuminuria in adults after prenatal exposure to the Dutch famine[J]. J Am Soc Nephrol, 2005, 16 (1): 189–194. |
| [14] | 智胜利. 糖尿病肾病尿蛋白与尿微量蛋白的检验结果分析[J]. 临床医药文献电子杂志, 2015, 2 (20): 4151. |
| [15] | Barker DJ, Winter PD, Osmond C, et al. Weight in infancy and death from ischaemic heart disease[J]. Lancet, 1989, 2 (8663): 577–580. |
| [16] | 黄文娟, 王成. 儿童原发性高血压的影响因素分析[J]. 中国小儿急救医学, 2015, 22 (9): 637–639. |
| [17] | Ponzio C, Palomino Z, Puccini RF, et al. Does low birth weight affect the presence of cardiometabolic risk factors in overweight and obese children[J]. Eur J Pediatr, 2013, 172 (12): 1687–1692. DOI:10.1007/s00431-013-2113-5 |
| [18] | Bilge I, Poyrazoglu S, Bas F, et al. Ambulatory blood pressure monitoring and renal functions in term small-for-gestational age children[J]. Pediatr Nephrol, 2011, 26 (1): 119–126. DOI:10.1007/s00467-010-1646-3 |
| [19] | Vehaskari VM, Aviles DH, Manning J. Prenatal programming of adult hypertension in the rat[J]. Kidney Int, 2001, 59 (1): 238–245. DOI:10.1046/j.1523-1755.2001.00484.x |