 2017, Vol. 19
2017, Vol. 19



儿童系统性红斑狼疮(juvenile-onset systemic lupus erythematosus, JSLE)是一种累及多系统的自身免疫性疾病。相比成年发病的SLE患者,JSLE患儿起病更快,严重程度高,死亡风险大[1]。过敏性鼻炎(allergic rhinitis, AR)是儿童常见的呼吸道变态反应性疾病。早在1976年,Goldman等[2]发现:相比正常人群,SLE患者更易合并过敏性鼻炎和药物过敏等过敏性疾病。最近台湾学者的研究显示,SLE患者特异性皮炎、过敏性鼻炎和哮喘的发生率约2倍多于非SLE对照组,其中与过敏性鼻炎之间的关联度较高[3]。但AR是否加重JSLE病情或影响其预后尚不清楚。为探讨AR对JSLE病情的影响以及对AR进行干预能否改善JSLE病情,本文对96例JSLE患儿进行对照研究,探讨AR对JSLE病情及治疗的影响。
1 资料与方法 1.1 研究对象以2005年10月至2015年6月期间上海交通大学医学院附属仁济医院儿科确诊的96例JSLE患儿为研究对象,均随访至少6个月。其中男性16例、女性80例。起病年龄2~16岁,确诊年龄11±3岁。96例患儿分为合并过敏性疾病组包括AR44例、非鼻炎过敏(哮喘、湿疹、过敏性结膜炎等)20例以及未合并过敏性疾病组32例。均根据《儿童风湿病学》[4]进行SLE规范治疗,44例合并AR的患儿随机分为鼻炎干预组和非干预组(各22例),干预组予以局部鼻喷剂(辅舒良或雷诺考特鼻喷雾剂)以及口服抗组胺(西替利嗪、开瑞坦、酮替芬、顺尔宁)药物治疗。本研究得到医院伦理委员会批准及患儿监护人知情同意。
1.2 JSLE、AR的诊断和病情评估JSLE诊断参照1997年美国风湿病学会修订的SLE诊断标准[5],均符合标准11项中的4项或以上,且除外感染、肿瘤和其他结缔组织病。AR的诊断及症状严重程度评价参考2010年儿童变应性鼻炎诊断和治疗指南[6]。JSLE病情评估采用SLE疾病活动指数(systemic lupus erythematosus disease activity index, SLEDAI)[7]衡量。糖皮质激素日累积剂量即将患儿所使用的激素量根据等效关系折算成甲泼尼龙量,并按照患儿单位体重进行计算。
1.3 统计学分析采用SPSS 20.0软件进行数据处理。符合正态分布的计量资料采用均数±标准差(x±s)表示,组间比较采用F检验或t检验;计数资料采用百分率(%)表示,组间比较采用χ2检验。P < 0.05为差异有统计学意义。
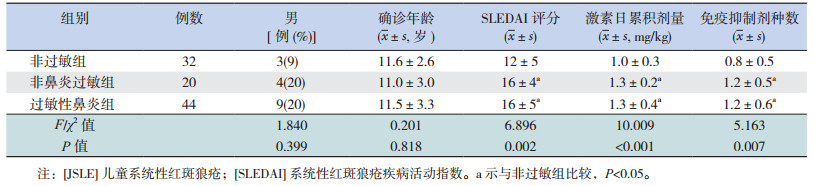
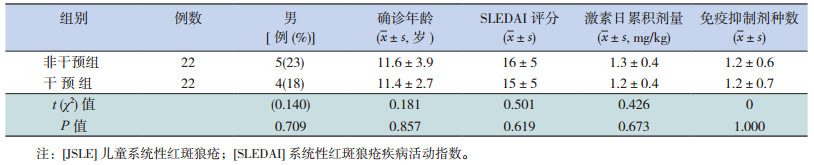
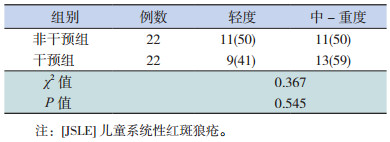
2 结果 2.1 各组JSLE患儿治疗前的一般资料、SLEDAI评分及用药情况比较与非过敏组比,治疗前SLEDAI评分、糖皮质激素日累积剂量、免疫抑制剂种数在合并AR和非AR过敏组的JSLE患儿较高(P < 0.05),而AR组和非AR过敏组间的差异无统计学意义(P > 0.05);3组患儿在性别构成比和确诊年龄的差异无统计学意义(P > 0.05)。见表 1。AR干预组与非干预组在性别构成比、确诊年龄,治疗前SLEDAI评分和鼻炎严重程度,以及激素或免疫抑制剂用药方面的差异均无统计学意义(P > 0.05),见表 2~3。
| 表 1 有无合并过敏性疾病的JSLE患儿一般资料、SLEDAI评分及用药情况比较 |
| 表 2 JSLE合并过敏性鼻炎患儿非干预组与干预组的一般资料、治疗前SLEDAI评分及用药情况比较 |
| 表 3 JSLE合并过敏性鼻炎非干预组与干预组治疗前鼻炎症状严重程度比较 [例(%)] |
2.2 JSLE合并AR的患儿治疗1个月后SLEDAI评分及用药情况比较
治疗1个月后,合并AR患儿鼻炎干预组的SLEDAI评分及激素日累积剂量低于非干预组(P < 0.05),两组在免疫抑制剂种数的差异无统计学意义(P > 0.05),见表 4。
| 表 4 JSLE合并过敏性鼻炎患儿非干预组与干预组治疗1个月后SLEDAI评分及用药情况比较(x±s) |
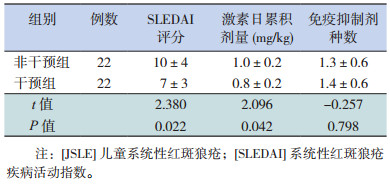
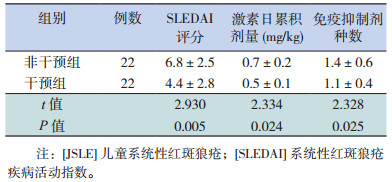
2.3 JSLE合并过敏性鼻炎患儿治疗3个月及6个月后SLEDAI评分及用药情况比较
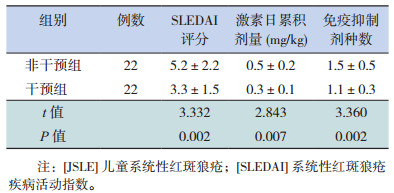
JSLE合并AR患儿治疗3个月及6个月后,鼻炎干预组的SLEDAI评分、激素日累积量、免疫抑制剂种数少于非干预组(P < 0.05),见表 5~6。
| 表 5 JSLE合并过敏性鼻炎非干预组与干预组治疗3个月后SLEDAI评分及用药情况比较(x±s) |
| 表 6 JSLE合并过敏性鼻炎非干预组与干预组治疗6个月后SLEDAI评分及用药情况比较(x±s) |
3 讨论
JSLE是一种慢性炎症性和多器官系统受累的自身免疫性疾病,常累及多脏器系统甚至危及生命[8]。近年研究发现,Th17细胞、调节性T细胞以及一些细胞因子在风湿性疾病和特应性疾病中起到不同的作用[9-10]。哮喘、过敏性鼻炎、结膜炎、变异性皮炎以及药物或食物过敏反应常发生于SLE患者[11],而伴发过敏性鼻炎等过敏性疾病是否对儿童SLE的病情及治疗产生影响报道甚少。
T辅助细胞(Th)和炎性细胞因子在自身免疫性疾病中的作用越来越受到重视,其中Th17(主要分泌IL17)和调节性T细胞(regulatory T cells, Treg)在自身免疫性疾病和过敏性疾病中起着重要作用。SLE患者血清IL-17水平明显升高,且能诱导自身抗体产生,在SLE发病机制中起关键作用[12]。有研究显示,AR患者外周血Th17细胞和IL-17水平明显高于健康对照,而升高的IL-17可加重JSLE病情,延缓其缓解[13]。目前认为,Treg细胞对自身免疫性疾病和过敏性疾病均有抑制作用。AR患者的外周血Treg低于健康对照[14],由此推测合并AR的JSLE患儿可能由于Treg细胞减少导致免疫抑制效应下降,病情加重或迁延不愈。Collison等[15]发现一种新的iTregs-iTr35调节细胞,通过IL-35介导其活性,而IL-35具有免疫抑制/抑炎作用。Cai等[16]发现,IL-35在SLE小鼠模型可致抗ANA抗体、抗ds-DNA抗体滴度下降,使SLE缓解。而丁莲富等[17]研究表明,AR患儿的血清IL-35水平低于健康儿童。由此推测合并AR的JSLE患儿可能因IL-35水平降低导致免疫反应增强,SLE病情加重。本研究发现伴发过敏性疾病的JSLE患儿治疗前的SLEDAI评分较高,糖皮质激素的日累积剂量较大,使用免疫抑制剂的种类也较多,与何珂骏等[18]研究一致。证实了合并特应质对JSLE病情及其治疗不利。进一步可行细胞因子检测以探讨其机制。
值得进一步思考的是,如何提高合并AR等特应质的风湿性疾病患儿疗效?近来研究发现,狼疮易感小鼠(MRL/lpr)的血清Th9细胞含量增加、IL-9水平升高,并与抗ds-DNA抗体滴度呈正相关,IL-9或IL-17的中和抗体可使MRL/lpr小鼠的抗ds-DNA抗体滴度下降、肾损伤减轻[19-20]。而Th9细胞及IL-9在AR患者中也明显升高,并与严重程度相关[21]。推测对于合并AR的JSLE患儿,减少IL-9分泌可能对预后有利。本研究合并AR的JSLE患儿在治疗原发病同时予以鼻炎干预者,治疗后1、3、6个月的SLEDAI评分、糖皮质激素日累积量均低于非干预组,免疫抑制剂的应用种类也少于非干预组。但机制是否与减少IL-9有关有待进一步研究。
综上,合并AR可能对JSLE病情及用药产生不利影响,进行AR的积极干预有利于JSLE控制。
| [1] | Chen YM, Lin CH, Chen HH, et al. Onset age affects mortality and renal outcome of female systemic lupus erythematosus patients:a nationwide population-based study in Taiwan[J]. Rheumatology (Oxford), 2014, 53 (1): 180–185. DOI:10.1093/rheumatology/ket330 |
| [2] | Goldman JA, Klimek GA, Ali R. Allergy in systemic lupus erythematosus. IgE levels and reaginic phenomenon[J]. Arthritis, Rheum, 1976, 19 (4): 669–676. DOI:10.1002/(ISSN)1529-0131 |
| [3] | Hsiao YP, Tsai JD, Muo CH, et al. Atopic diseases and systemic lupus erythematosus:an epidemiological study of the risks and correlations[J]. Int J Environ Res Public Health, 2014, 11 (8): 8112–8122. DOI:10.3390/ijerph110808112 |
| [4] | 李博, 叶志中. 系统性红斑狼疮[M]//叶志中, 李博, 何伟珍. 儿童风湿病学. 北京: 人民卫生出版社, 2009: 193-214. |
| [5] | Kuhn A, Bonsmann G, Anders HJ, et al. The diagnosis and treatment of systemic lupus erythematosus[J]. Dtsch Arztebl Int, 2015, 112 (25): 423–432. |
| [6] | 中华耳鼻咽喉头颈外科杂志编辑委员会鼻科组, 中华医学会耳鼻咽喉头颈外科学分会鼻科学组、小儿学组, 中华儿科杂志编辑委员会. 儿童变应性鼻炎诊断和治疗指南 (2010年, 重庆)[J]. 中华耳鼻咽喉头颈外科杂志, 2011, 46 (1): 7–8. |
| [7] | Rao V, Gordon C. Advances in the assessment of lupus disease activity and damage[J]. Curr Opin Rheumatol, 2014, 26 (5): 510–519. DOI:10.1097/BOR.0000000000000085 |
| [8] | Tavangar-Rad F, Ziaee V, Moradinejad MH, et al. Morbidity and mortality in Iranian children with juvenile systemic lupus erythematosus[J]. Iran J Pediatr, 2014, 24 (4): 365–370. |
| [9] | Wilke CM, Bishop K, Fox D, et al. Deciphering the role of Th17 cells in human disease[J]. Trends Immunol, 2011, 32 (12): 603–611. DOI:10.1016/j.it.2011.08.003 |
| [10] | Akdis M, Burgler S, Crameri R, et al. Interleukins, from 1 to 37, and interferon-γ:receptors, functions, and roles in diseases[J]. J Allergy Clin Immunol, 2011, 127 (3): 701–721.e70. DOI:10.1016/j.jaci.2010.11.050 |
| [11] | Shen TC, Tu CY, Lin CL, et al. Increased risk of asthma in patients with systemic lupus erythematosus[J]. Am J Respir Crit Care Med, 2014, 189 (4): 496–499. DOI:10.1164/rccm.201310-1792LE |
| [12] | Martin JC, Baeten DL, Josien R. Emerging role of IL-17 and Th17 cells in systemic lupus erythematosus[J]. Clin Immunol, 2014, 154 (1): 1–12. DOI:10.1016/j.clim.2014.05.004 |
| [13] | Xuekun H, Qintai Y, Yulian C, et al. Correlation of gammadelta-T-cells, Th17 cells and IL-17 in peripheral blood of patients with allergic rhinitis[J]. Asian Pac J Allergy Immunol, 2014, 32 (3): 235–239. |
| [14] | 黄雪琨, 杨钦泰, 陈玉莲, 等. γδ T细胞、调节性T细胞、白细胞介素17及转化生长因子β1在变应性鼻炎患者外周血中的表达[J]. 中华耳鼻咽喉头颈外科杂志, 2013, 48 (7): 544–548. |
| [15] | Collison LW, Workman CJ, Kuo TT, et al. The inhibitory cytokine IL-35 contributes to regulatory T-cell function[J]. Nature, 2007, 450 (7169): 566–569. DOI:10.1038/nature06306 |
| [16] | Cai Z, Wong CK, Dong J, et al. Remission of systemic lupus erythematosus disease activity with regulatory cytokine interleukin (IL)-35 in Murphy Roths Large (MRL)/lpr mice[J]. Clin Exp Immunol, 2015, 181 (2): 253–266. DOI:10.1111/cei.12639 |
| [17] | 丁莲富, 陈强, 李岚, 等. 舌下特异性免疫治疗过敏性鼻炎/过敏性哮喘患儿IL-17和IL-35水平的变化及临床疗效[J]. 中国当代儿科杂志, 2014, 16 (12): 1206–1210. DOI:10.7499/j.issn.1008-8830.2014.12.004 |
| [18] | 何珂骏. 特应性体质对常见儿童风湿病病情的影响[D]. 上海: 上海交通大学, 2009. |
| [19] | Leng RX, Pan HF, Ye DQ, et al. Potential roles of IL-9 in the pathogenesis of systemic lupus erythematosus[J]. Am J Clin Exp Immunol, 2012, 1 (1): 28–32. |
| [20] | Yang J, Li Q, Yang X, et al. Interleukin-9 is associated with elevated anti-double-stranded DNA antibodies in lupus-prone mice[J]. Mol Med, 2015, 21 : 364–370. |
| [21] | Wang XQ, Hu GH, Kang HY, et al. High frequency of T helper type 9 cells in Chinese patients with allergic rhinitis[J]. Asian Pac J Allergy Immunol, 2015, 33 (4): 301–307. |