 2017, Vol. 19
2017, Vol. 19



哮喘是儿童常见的慢性肺部疾病,目前在全球不同国家发病率为1%~18%[1],呈逐年上升趋势。我国儿童哮喘现患率、累积患病率及肥胖、超重的检出率在数十年内均明显增长[2-3]。多个研究显示肥胖与哮喘相关[4-10],但机制至今尚未明确。2014年全球哮喘处理和预防策略(GINA)提出了伴有肥胖的哮喘这一常见表型[1]。有研究表明,肥胖与哮喘的关系受年龄[6, 11]、性别[9, 12-13]等因素的影响,但尚未见评估肥胖对我国学龄前及学龄期哮喘患儿肺功能影响是否存在差异的研究。本研究通过分析学龄前及学龄期不同体重指数(BMI)哮喘患儿的肺功能,探讨肥胖对儿童哮喘的影响在此两年龄段存在的差异。
1 资料与方法 1.1 研究对象研究对象为2014年9月至2016年5月于重庆医科大学附属儿童医院哮喘专科门诊就诊的初诊哮喘患儿294例。年龄3.1~12.5岁。按年龄分为学龄前期组( < 6岁)和学龄期组(6~12.5岁)。学龄前期组179人,平均年龄4.4±0.7岁;学龄期组115人,平均年龄8.0±1.5岁。两组患儿按我国0~18岁BMI肥胖、超重筛查界值点的方法[14],分为正常体重哮喘组、超重哮喘组及肥胖哮喘组。其中学龄前期组中,正常体重82例(45.8%,BMI:15.3±0.8 kg/m2)、超重43例(24.0%,BMI:17.0±0.3 kg/m2),肥胖54例(30.2%,BMI:19.1±1.7 kg/m2);学龄期组中,正常体重56例(48.7%,BMI:15.7±1.4 kg/m2),超重25例(21.7%,BMI:18.8±1.3 kg/m2),肥胖34例(29.6%,BMI:21.7±2.5 kg/m2)。
研究对象纳入标准:(1)符合中华医学会儿科学分会呼吸学组修订的儿童哮喘诊断标准[15];(2)年龄 > 3岁;(3)诊断时完善肺功能检查,均为稳定期轻、中度哮喘患儿[15]。
排除标准:(1)3周内有呼吸道感染;(2)哮喘急性发作;(3)先天性心肺发育畸形或异常、胸廓畸形;(4)患神经肌肉疾病;(5)已行糖皮质激素治疗、长期口服或静脉使用激素者。
1.2 肺功能检测均采用常规通气法检测肺功能,具体检测方法见本课题组叶泽慧等[16]的文章。观察指标:用力肺活量(FVC)、第1秒用力呼气量(FEV1)、用力呼气25%流量(MEF25)、用力呼气50%流量(MEF50)、用力呼气75%流量(MEF75)的实测值占预计值的百分比。
1.3 统计学分析采用SPSS 21.0软件进行统计学分析。计数资料用例数和百分率(%)表示,计量资料用均数±标准差(x±s)表示。校正混杂因素后组间比较采用一般线性模型单变量分析,P < 0.05为差异有统计学意义。
2 结果 2.1 两年龄组间基础肺功能的比较在校正了性别及BMI分组因素后,学龄期组FEV1%、MEF25%、MEF50%明显低于学龄前期组,差异有统计学意义(P < 0.05),见表 1。
| 表 1 两年龄组间基础肺功能的比较(x±s) |

2.2 两年龄组间不同BMI状态下肺功能的比较
两年龄组正常体重患儿间比较,学龄期组基础肺功能FEV1%、MEF25%、MEF50%低于学龄前期组,差异有统计学意义(P < 0.05), 见表 2。两年龄组超重患儿间比较,FVC%及MEF50%差异有统计学意义(P < 0.05),亦为学龄期组低于学龄前期组,见表 3。而两年龄组肥胖患儿间比较,肺功能各指标差异均无统计学意义,见表 4。
| 表 2 两年龄组体重正常患儿肺功能的比较(x±s) |

| 表 3 两年龄组超重患儿肺功能的比较(x±s) |

| 表 4 两年龄组肥胖患儿肺功能的比较(x±s) |

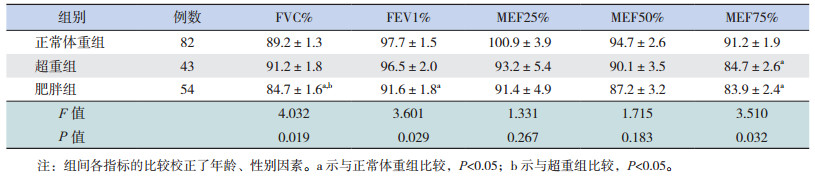
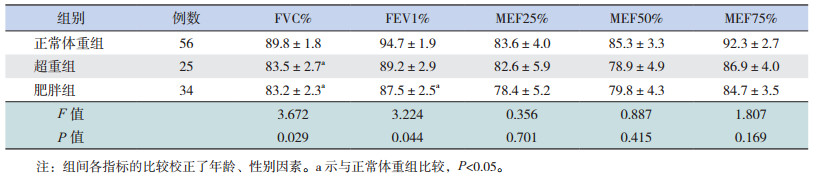
2.3 不同年龄段不同BMI组间基础肺功能的比较
学龄前期患儿中,肥胖组基础肺功能FVC%、FEV1%、MEF75%低于正常体重组,FVC%低于超重组;超重组基础肺功能MEF75%亦较正常体重组低,差异均有统计学意义(P < 0.05),见表 5。学龄期患儿中,肥胖组肺功能FVC%、FEV1%低于正常体重组,超重组FVC%亦低于正常体重组,差异均有统计学意义(P < 0.05),见表 6。
| 表 5 学龄前期不同BMI组间基础肺功能的比较(x±s) |
| 表 6 学龄期不同BMI组间基础肺功能的比较(x±s) |
3 讨论
哮喘与肥胖的发病率均呈逐年上升趋势,肥胖作为儿童哮喘的一个危险因素已被很多研究提出[7, 13, 17]。但至今超重及肥胖对哮喘患儿肺功能的影响仍存在较多争议,对不同年龄段初诊哮喘患儿肺功能的研究较少。Holguin等[18]研究早发及晚发哮喘与肥胖的关系,发现随着BMI的升高,二者肺功能均呈下降趋势,同时升高的BMI在小年龄早发哮喘患儿还与哮喘持续时间相关。而Mahut等[19]观察到肺功能与BMI的关系并不与哮喘特定相关。
本研究中两个不同年龄组间基础肺功能比较结果显示,学龄期组大小气道通气功能指标(FVC%、FEV1%、MEF75%)低于学龄前期组。Lang等[11]研究显示,随着年龄的增长,哮喘患者肺功能FEV1%及FEV1/FVC降低,本研究结果与之类似,但目前机制尚不明确。本研究进一步行两年龄组间同一体质状态下肺功能的比较,发现同为正常体重的两年龄组患儿,学龄前期组大小气道通气功能更好,但随着BMI的增加,两年龄组间肺功能差异减小,考虑与肥胖对小年龄患儿肺功能的影响程度更大有关,即肥胖状态下,学龄前期组肺功能下降值较学龄期组高。本研究亦显示,学龄前期肥胖组大小气道通气功能指标(FVC%、FEV1%、MEF75%)均低于体重正常组,而学龄期肥胖组仅大气道通气功能指标(FVC%、FEV1%)低于体重正常组,说明肥胖对哮喘肺功能的影响在不同年龄段组间存在差异,一定程度上对学龄前期患儿影响更大,即随着年龄的增长,哮喘与肥胖的关系表现得越弱,与Lang等[11]及Holguin等[18]的研究结果类似,推测与随着年龄的增长,儿童全身脂肪比例下降有关,同时年龄越小,膈肌及肺等呼吸器官发育越不完全,受肥胖生理、机械等作用的影响越大。Holguin等[18]研究还发现小年龄肥胖哮喘患儿的气道阻力及血清IgE水平较大年龄肥胖患儿高,这可能也是小年龄肥胖患儿肺功能下降更明显的原因。
本研究结果还表明,两个不同年龄段肥胖组基础肺功能均较体重正常组差,超重组与体重正常组比较亦存在差异,但无肥胖组明显,说明超重及肥胖能够限制哮喘患儿气道通气功能,且随着BMI的升高其影响逐渐增大,与Mitchell等[8]、Spathopoulos等[20]及Chih等[21]的研究一致。Beuther[17]在其综述中也提出肥胖与哮喘存在因果、剂量关系。肥胖,特别是向心性肥胖,致膈肌上抬肺容积减少,膈肌活动、肺扩张受限,气道口径缩小,从而增加气道阻力[22]。同时肥胖患儿的气道平滑肌缩短、效率下降,通过肌丝-横桥周期机制致气道口径缩小或关闭、肺顺应性及气道表面张力降低,使肺不易扩张,从而影响基础肺功能并导致通气需求增加[23-24]。Chih等[21]研究亦证实了肺功能下降是中央型肥胖相关哮喘最为重要的介导通路。此外,肥胖哮喘患儿存在的生化改变,如瘦素、脂联素、白细胞介素-6、TNF-α等细胞炎症因子在外周循环的升高,导致气道炎症增加,对气道结构及功能的改变也存在影响[6, 17, 23-24]。
综上所述,本研究显示了肥胖对哮喘患儿肺功能的影响,以及这种影响在不同年龄段间存在差异,其对学龄前患儿影响更大。本研究为不同年龄段肥胖哮喘儿童的临床治疗和评估提供了参考,但本研究样本量偏小,且研究对象并未包括青春期及以后、甚至成人,要进一步探索肥胖与年龄对哮喘的影响、在不同年龄间存在的差异及相关机制,还需要多中心不同年龄段大样本的临床及基础研究。
| [1] | Global Initiative for Asthma. Global strategy for asthma management and prevention[EB/OL]. (May 2014). http:www.ginasthma.org. |
| [2] | 马冠生, 李艳平, 武阳丰, 等. 1992至2002年间中国居民超重率和肥胖率的变化[J]. 中华预防医学杂志, 2005, 39 (5): 311–315. |
| [3] | 全国儿科哮喘协作组, 中国疾病预防控制中心环境与健康相关产品安全所. 第三次中国城市儿童哮喘流行病学调查[J]. 中华儿科杂志, 2013, 51 (10): 729–735. DOI:10.3760/cma.j.issn.0578-1310.2013.10.003 |
| [4] | Forno E, Lescher R, Strunk R, et al. Decreased response to inhaled steroids in overweight and obese asthmatic children[J]. J Allergy Clin Immunol, 2011, 127 (3): 741–749. DOI:10.1016/j.jaci.2010.12.010 |
| [5] | Simard B, Turcotte H, Marceau P, et al. Asthma and sleep apnea in patients with morbid obesity:outcome after bariatric surgery[J]. Obes Surg, 2004, 14 (10): 1381–1388. DOI:10.1381/0960892042584021 |
| [6] | Papoutsakis C, Priftis KN, Drakouli M, et al. Childhood overweight/obesity and asthma:is there a link? A systematic review of recent epidemiologic evidence[J]. J Acad Nutr Diet, 2013, 113 (1): 77–105. DOI:10.1016/j.jand.2012.08.025 |
| [7] | Liu PC, Kieckhefer GM, Gau BS. A systematic review of the association between obesity and asthma in children[J]. J Adv Nurs, 2013, 69 (7): 1446–1465. DOI:10.1111/jan.12129 |
| [8] | Mitchell EA, Beasley R, Björkstén B, et al. The association between BMI, vigorous physical activity and television viewing and the risk of symptoms of asthma, rhinoconjunctivitis and eczema in children and adolescents:ISAAC Phase Three[J]. Clin Exp Allergy, 2013, 43 (1): 73–84. DOI:10.1111/cea.2012.43.issue-1 |
| [9] | Chen YC, Dong GH, Lin KC, et al. Gender difference of childhood overweight and obesity in predicting the risk of incident asthma:a systematic review and meta-analysis[J]. Obes Rev, 2013, 14 (3): 222–231. DOI:10.1111/obr.2013.14.issue-3 |
| [10] | Lang JE, Hossain J, Smith K, et al. Asthma severity, exacerbation risk, and controller treatment burden in underweight and obese children[J]. J Asthma, 2012, 49 (5): 456–463. DOI:10.3109/02770903.2012.677895 |
| [11] | Lang JE, Hossain J, Dixon AE, et al. Does age impact the obese asthma phenotype? Longitudinal asthma control, airway function, and airflow perception among mild persistent asthmatics[J]. Chest, 2011, 140 (6): 1524–1533. DOI:10.1378/chest.11-0675 |
| [12] | Lang JE, Holbrook JT, Wise RA, et al. Obesity in children with poorly controlled asthma:Sex differences[J]. Pediatr Pulmonol, 2013, 48 (9): 847–856. DOI:10.1002/ppul.22707 |
| [13] | Gold DR, Damokosh AI, Dockery DW, et al. Body-mass index as a predictor of incident asthma in a prospective cohort of children[J]. Pediatr Pulmonol, 2003, 36 (6): 514–521. DOI:10.1002/(ISSN)1099-0496 |
| [14] | 李辉, 季成叶, 宗心南, 等. 中国0~18岁儿童、青少年体块指数的生长曲线[J]. 中华儿科杂志, 2009, 47 (7): 745–753. |
| [15] | 中华医学会儿科学分会呼吸学组. 儿童支气管哮喘诊断与防治指南 (2016年版)[J]. 中华儿科杂志, 2016, 54 (3): 167–181. |
| [16] | 叶泽慧, 黄英, 王莹, 等. 不同体重指数的哮喘患儿规范化激素治疗后肺功能变化[J]. 中国当代儿科杂志, 2013, 15 (11): 983–986. DOI:10.7499/j.issn.1008-8830.2013.11.014 |
| [17] | Beuther DA. Recent insight into obesity and asthma[J]. Curr Opin Pulm Med, 2010, 16 (1): 64–70. DOI:10.1097/MCP.0b013e3283338fa7 |
| [18] | Holguin F, Bleecker ER, Busse WW, et al. Obesity and asthma:An association modified by age of asthma onset[J]. J Allergy Clin Immunol, 2011, 127 (6): 1486–1493.e2. DOI:10.1016/j.jaci.2011.03.036 |
| [19] | Mahut B, Beydon N, Delclaux C. Overweight is not a comorbidity factor during childhood asthma:the GrowthOb study[J]. Eur Respir J, 2012, 39 (5): 1120–1126. DOI:10.1183/09031936.00103311 |
| [20] | Spathopoulos D, Paraskakis E, Trypsianis G, et al. The effect of obesity on pulmonary lung function of school aged children in Greece[J]. Pediatr Pulmonol, 2009, 44 (3): 273–280. DOI:10.1002/ppul.v44:3 |
| [21] | Chih AH, Chen YC, Tu YK, et al. Mediating pathways from central obesity to childhood asthma:a population-based longitudinal study[J]. Eur Respir J, 2016, 48 (3): 748–757. DOI:10.1183/13993003.00226-2016 |
| [22] | King GG, Brown NJ, Diba C, et al. The effects of body weight on airway calibre[J]. Eur Respir J, 2005, 25 (5): 896–901. DOI:10.1183/09031936.05.00104504 |
| [23] | Shore SA. Obesity and asthma:possible mechanisms[J]. J Allergy Clin Immunol, 2008, 121 (5): 1087–1093. DOI:10.1016/j.jaci.2008.03.004 |
| [24] | Beuther DA. Obesity and asthma[J]. Clin Chest Med, 2009, 30 (3): 479–488. DOI:10.1016/j.ccm.2009.05.002 |