PDF(1464 KB)
PDF(1464 KB)

Effects of nosocomial infection trends on neonatal outcomes in preterm infants <33 weeks of gestational age in Canadian NICUs
Caitlin Jantzen, Abhay Lodha, Mirea Lucia, Shoo K Lee, Xiang Y Ye, Koravangattu Sankaran
Chinese Journal of Contemporary Pediatrics ›› 2015, Vol. 17 ›› Issue (10) : 1019-1027.
PDF(1464 KB)
PDF(1464 KB)
Effects of nosocomial infection trends on neonatal outcomes in preterm infants <33 weeks of gestational age in Canadian NICUs
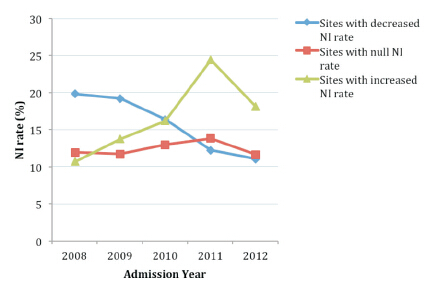
Objective To characterize recent trends of nosocomial infection (NI) among preterm infants admitted to Canadian Level 3 NICUs during 2008-2012, and its association with neonatal outcomes. Methods A retrospective observational cohort study was performed including infants born <33 weeks gestational age and admitted to 24 NICU sites participating in the Canadian Neonatal NetworkTM during 2008-2012. NICU sites were classified into three groups according to their baseline NI rates in 2008 [Low NI group (≤14%), Medium NI group (14.1%-19%) and High NI group (>19% )], and NICU sites were also classified according to their NI trend during 2008-2012 (decreased, null and increased). Trends in NI were further examined for each baseline-NI group. Trends for a composite outcome indicating mortality or severe morbidities (intraventricular hemorrhage grades ≥3 or periventricular leukomalacia, retinopathy of prematurity stages ≥3, bronchopulmonary dysplasia or necrotizing enterocolitis stages ≥2) were examined for each baseline-NI and trend-NI NICU site groups using multivariable logistic regression analyses adjusted for potential confounders. Results Baseline high NI group showed significantly decreased trends in NI rates, while for with medium or low baseline NI groups showed no significant trends in NI rates. The composite outcome (mortality during NICU stay or any severe neonatal morbidity such as intraventricular hemorrhage grades 3-4, periventricular leukomalacia, retinopathy of prematurity stages 3-5, bronchopulmonary dysplasia and necrotizing enterocolitis stages 2-3) decreased significantly for sites with decreased (OR=0.89, 95% CI=0.85-0.93) or null (OR=0.94, 95% CI=0.90-0.98) NI trends, but no significant trends in the composite outcome were detected for sites with increased NI rates. Conclusions The neonatal outcome is possibly influenced by NI rates and trend. The trend in the mortality and the risk of bronchopulmonary dysplasia, retinopathy of prematurity stage ≥3 and intraventricular hemorrhage >2 were significantly decreased for sites with decreased NI trend, suggesting that these improved outcomes may be associated with effort to decrease NI rate.