目的:总结分析杜兴型肌营养不良(Duchenne muscular dystrophy, DMD)患儿的临床及病理特点,旨在加强对DMD的认识,提高DMD的早期诊断率。方法:对50例通过临床表现、骨骼肌活检并进行单克隆抗体免疫组化染色确诊的DMD患儿的临床资料进行回顾性分析。结果:DMD患儿临床表现为:自幼跑步慢,爬楼、蹲起费力,逐渐出现走路姿势异常,检查发现肌酸激酶显著增高,肌电图呈肌源性损害。组织化学染色显示:50例患儿苏木精-伊红染色均可见肌纤维大小不一,圆形化,肌纤维明显变性、坏死,肌纤维不同程度再生,结缔组织增生;部分肌纤维间可见少量炎性细胞浸润。免疫组织化学染色显示:50例患儿均可见肌纤维膜dystrophins蛋白表达完全缺失,33例患儿肌纤维膜sarcoglycans(-α,-β,-γ,-δ)不同程度表达减弱。结论:对具有上述临床表现的患儿,建议行骨骼肌活检并进行单克隆抗体免疫组化染色,发现肌细胞膜上dystrophins蛋白缺失即可确诊DMD。
Abstract
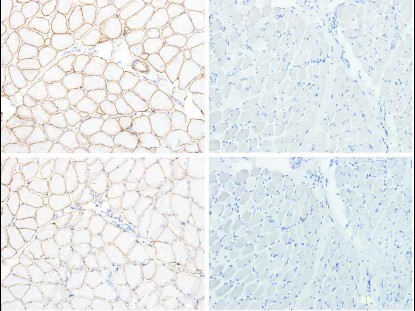
OBJECTIVE: To study the clinical and pathological features of children with Duchenne muscular dystrophy (DMD), with the aim of increasing the possibility of early diagnosis. METHODS: The clinical data of 50 children who were definitely diagnosed with DMD, based on clinical manifestations and the results of skeletal muscle biopsies and monoclonal antibody immunohistochemical staining, was reviewed. RESULTS: The children showed similar clinical manifestations, including running slowly in the toddler period, muscle weakness when climbing stairs and standing up followed by squatting down and walking abnormalities a predominant increase in serum creatine kinase level increased dominantly, and myopathic lesions seen on electromyography. Hematoxylin-eosin staining showed similar pathological presentations in all 50 children, including differentsized muscle fibers with rounding, degeneration and necrosis in various degrees, and proliferation of connective tissues. There was some inflammatory cell infiltration in muscle fibers and interstitial tissues. Dystrophin expression was completely absent at the sarcolemma in all 50 children, and sarcoglycan-α,-β, -γ,-δ expression was reduced to various degrees in 33 of them. CONCLUSIONS: For children with the clinical manifestations mentioned above, skeletal muscle biopsies and monoclonal antibody immunohistochemical staining are recommended as these examinations contribute to a definite diagnosis of DMD by demonstrating dystrophin deficiency at the sarcolemma.
关键词
杜兴型肌营养不良 /
骨骼肌活检 /
肌酸激酶 /
免疫组织化学染色 /
Dystrophin蛋白 /
儿童
Key words
Duchenne muscular dystrophy /
Skeletal muscle biopsy /
Creatine kinase /
Immunohistochemistry staining /
Dystrophin /
Child
{{custom_sec.title}}
{{custom_sec.title}}
{{custom_sec.content}}
参考文献
[1]胡静.骨骼肌疾病临床病理诊断[M]. 北京:人民卫生出版社,2011:1-274.
[2]Cohn RD, Campbell KP. Molecular basis of muscular dystrophies[J]. Muscle Nerve, 2000, 23(10): 1456-1471.
[3]Kunkel LM, Monaco AP, Middlesworth W, Ochs HD, Latt SA. Specific cloning of DNA fragments absent from the DNA of a male patient with an X chromosome deletion[J]. Proc Natl Acad Sci U S A, 1985, 82(14): 4778-4782.
[4]申本昌, 张成, 陈松林,孙筱放,李少英,姚晓黎,等.非缺失/重复型Duchenne肌营养不良症患者的致病点突变分析[J].中华医学遗传学杂志, 2006, 23(4) : 392-396.
[5]Ray PN, Belfall B, Duff C, Logan C, Kean V, Thompson MW, et al. Cloning of the breakpoint of an X; 21 translocation associated with Duchenne muscular dystrophy[J]. Nature, 1985, 318 (6047): 672-675.
[6]胡静,袁军辉,李娜,赵哲,沈宏锐,梅丽,刘彦. dysferlinopathy患者八例临床及分子病理学特点[J].中华神经科杂志, 2007, 40(12): 807-811.
[7]Petrof BJ. Molecular pathophysiology of myofiber injury in deficiencies of the dystrophin-glycoprotein complex[J]. Am J Phys Med Rehabil, 2002, 81(11 Suppl): S162-S174.
[8]Kakulas BA. The differential diagnosis of the human dystrophinopathies and related disorders[J]. Curr Opin Neurol, 1996, 9(5): 380-388.
[9]Fairclough RJ, Bareja A, Davies KE. Progress in therapy for Duchenne muscular dystrophy [J]. Exp Physiol, 2011, 96(11): 1101-1113.
 PDF(1412 KB)
PDF(1412 KB)