PDF(1185 KB)
PDF(1185 KB)

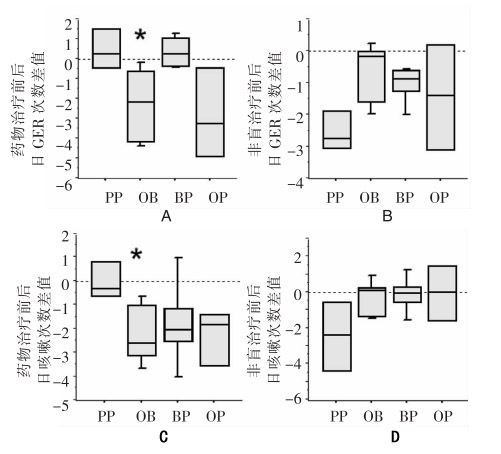
婴幼儿胃食管反流相关性咳嗽治疗的初步研究
Darryl J. Adamko, Carina M. Majaesic, Christopher Skappak, Adrian B. Jones
中国当代儿科杂志 ›› 2012, Vol. 14 ›› Issue (5) : 321-327.
PDF(1185 KB)
PDF(1185 KB)
婴幼儿胃食管反流相关性咳嗽治疗的初步研究
A pilot trial on the treatment of gastroesophageal reflux-related cough in infants