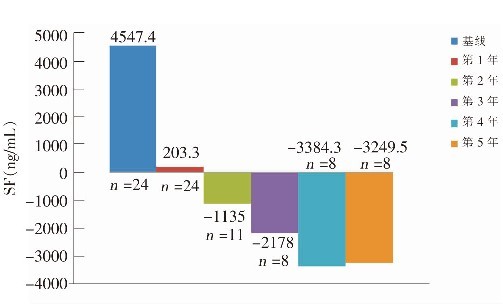
目的:探讨铁螯合剂地拉罗司(deferasirox,DFX)治疗重型β-地中海贫血(β-thalassemia major,β-TM)铁过载患儿的疗效及安全性。方法随机选择24例规律输血的β-TM铁过载患儿,参加DFX不同服药剂量的临床研究,调查血清铁蛋白(SF)的变化及不良反应。并将持续服用DFX 5年患儿与同期使用去铁胺联合去铁酮治疗患儿(对照组)的心脏MRI T2*、肝脏MRI T2*值进行比较。结果DFX每日20~30 mg/kg的起始剂量对于铁过载患儿无明显效果,加量至每日30~40 mg/kg 后SF水平下降显著(U=58,P<0.01);不良反应以血清肝脏转氨酶升高最为常见,其次为血清肌酐非进行性升高。持续DFX 治疗5年组SF水平明显低于对照组(1748±481 ng/mL vs 3462±1744 ng/mL,P<0.05);肝脏MRI T2* 值明显高于对照组(8.5±2.9 ms vs 2.7±1.9 ms,P<0.01)。两组心脏MRI T2*均值比较差异无统计学意义。结论DFX能显著降低β-TM 患儿SF水平,并显示出剂量依赖性变化;其对心脏铁负荷的减少未显示出明显优势,而对肝脏铁负荷的减低疗效显著。DFX治疗的不良反应以肝酶升高、血清肌酐非进行性升高为主。
Abstract
OBJECTIVE: To study the effectiveness and safety of deferasirox (DFX) in the treatment of iron overload in children with β-thalassemia major. METHODS: Twenty-four β-thalassemia major children with iron overload who received regular blood transfusion were randomly enrolled. The serum feritin (SF) levels were measured in the patients after different doses of DFX treatment. The DFX treatment-related adverse events were observed. The values of cardiac MRI T2* and liver MRI T2* were compared between the patients receiving DFX treatment for 5 years and the patients treated with deferoxamine and deferiprone. RESULTS: The patients with iron overload did not respond to DFX at the initial dose of 20-30 mg/kg?d. However, the SF level decreased significantly after the dose of DFX increased to 30-40 mg/kg?d (U=58, P<0.01). Serum liver transaminase elevation was the most common adverse effect, followed by non-progressive elevation in serum creatinine level. The mean SF level was significantly lower (1748±481 ng/mL vs 3462±1744 ng/mL; P<0.05), in contrast, the liver MRI T2* value was significantly higher (8.5±2.9 ms vs 2.7±1.9 ms; P<0.01) in patients receiving DFX treatment for 5 years than in the controls. There were no significant differences in the cardiac MRI T2* value between the two groups. CONCLUSIONS: DFX can reduce SF levels in a dose-dependent manner in children with β-thalassemia major. It can significantly lower liver iron overload but not cardiac overload. Serum liver transaminase elevation and non-progressive elevation in serum creatinine level are major adverse effects in DFX treatment.
关键词
重型β-地中海贫血 /
地拉罗司 /
血清铁蛋白 /
铁负荷 /
儿童
Key words
β-thalassemia major /
Deferasirox /
Serum feritin /
Iron overload /
Child
{{custom_sec.title}}
{{custom_sec.title}}
{{custom_sec.content}}
参考文献
[1]麦惠容,李长钢,王缨,石红松,赵维玲,陈运生,等.不同基因型地中海贫血患儿铁代谢和红细胞系造血状况研究[J].中国当代儿科杂志,2010,12(8):602-604.
[2]胡亚美,江载芳.诸福棠实用儿科学[M].第7版.北京:人民卫生出版社,2002:1763-1772.
[3]方建培,徐宏贵.重型β地中海贫血的输血和除铁治疗[J].中国小儿血液,2005,10(5):234-237.
[4]Au WY, Lam WW, Chu WW, Yuen HL, Ling AS, Li RC, et al. A cross-sectional magnetic resonance imaging assessment of organ specific hemosiderosis in 180 thalassemia major patients in Hong Kong[J]. Haematologica, 2008, 93(5):784-786.
[5]Anderson LJ, Holden S, Davis B, Prescott E, Charrier CC, Bunce NH, et al. Cardiovascular T2-star(T2*) magnetic resonance for the early diagnosis of myocardial iron overload[J]. Eur Heart J, 2001, 22(23): 2171-2179.
[6]Pennell DJ, Porter JB, Cappellini MD, Chan LL, El-Beshlawy A, Aydinok Y, et al. Continued improvement in myocardial T2* over two years of deferasirox therapy in β-thalassemia major patients with cardiac iron overload[J]. Haematologica, 2011, 96(1):48-54.
[7]Cappellini MD. Iron-chelating therapy with the new oral agent ICL670 (Exjade) [J].Best Pract Res Clin Haematol, 2005, 18(2):289-298.
[8]Cappellini MD, Porter J, El-Beshlawy A, Li CK, Seymour JF, Elalfy M, et al. Tailoring iron chelation by iron intake and serum ferritin: the prospective EPIC study of deferasirox in 1744 patients with transfusion-dependent anemias[J]. Haematologica, 2010, 95 (4):557-566.
[9]Borgna-Pignatti C, Rugolotto S, De Stefano P, Zhao H, Cappellini MD, Del Vecchio GC, et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine[J]. Haematologica, 2004, 89(10):1187-1193.
[10]Atiq M, Bana M, Ahmed US, Bano S, Yousuf M, Fadoo Z, et al.Cardiac disease in beta-thalassaemia major: is it reversible?[J]. Singapore Med J, 2006, 47(8):693-696.
 PDF(1078 KB)
PDF(1078 KB)